

How health service delivery guides the allocation of major trauma patients in the intensive care units of the inclusive (hub and spoke) trauma system of the Emilia Romagna Region (Italy). A cross-sectional study
- PMID: 28965094
- PMCID: PMC5640142
- DOI: 10.1136/bmjopen-2017-016415
How health service delivery guides the allocation of major trauma patients in the intensive care units of the inclusive (hub and spoke) trauma system of the Emilia Romagna Region (Italy). A cross-sectional study
Abstract
Objective: To evaluate cross-sectional patient distribution and standardised 30-day mortality in the intensive care units (ICU) of an inclusive hub and spoke trauma system.
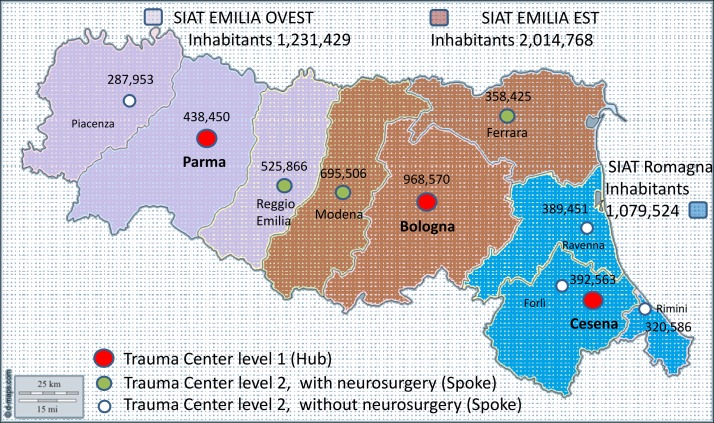
Setting: ICUs of the Integrated System for Trauma Patient Care (SIAT) of Emilia-Romagna, an Italian region with a population of approximately 4.5 million.
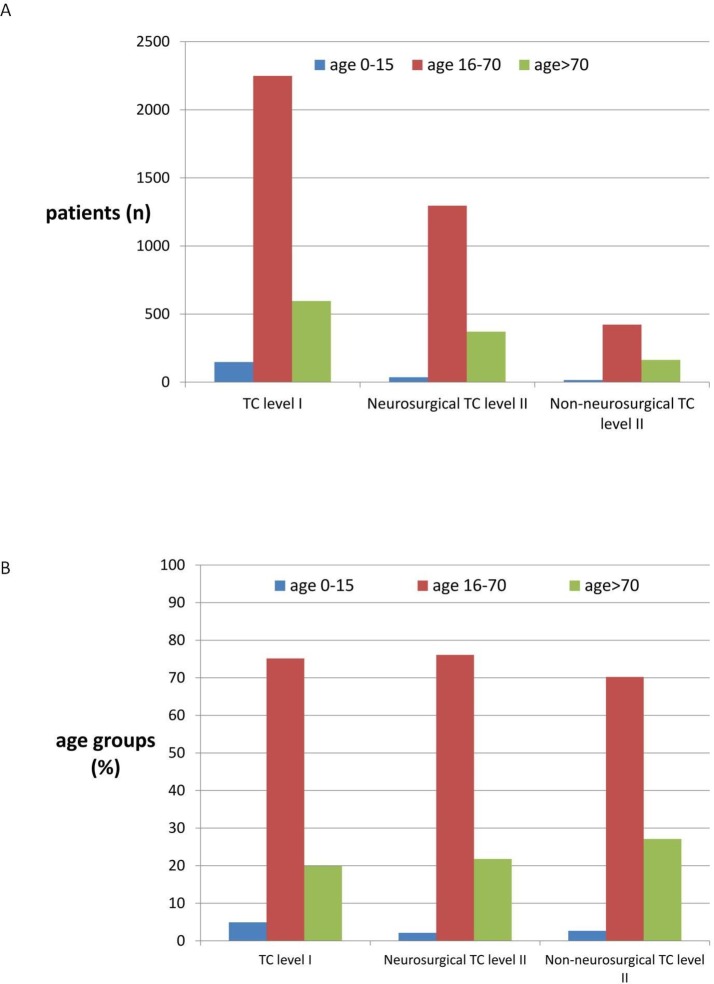
Participants: 5300 patients with an Injury Severity Score (ISS) >15 were admitted to the regional ICUs and recorded in the Regional Severe Trauma Registry between 2007 and 2012. Patients were classified by the Abbreviated Injury Score as follows: (1) traumatic brain injury (2) multiple injuriesand (3) extracranial lesions. The SIATs were divided into those with at least one neurosurgical level II trauma centre (TC) and those with a neurosurgical unit in the level I TC only.
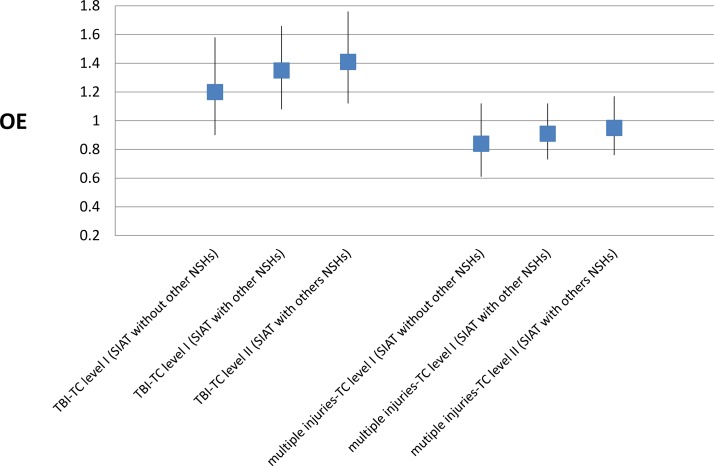
Results: A higher proportion of patients (out of all SIAT patients) were admitted to the level I TC at the head of the SIAT with no additional neurosurgical facilities (1083/1472, 73.6%) compared with the level I TCs heading SIATs with neurosurgical level II TCs (1905/3815; 49.9%). A similar percentage of patients were admitted to level I TCs (1905/3815; 49.9%) and neurosurgical level II TCs (1702/3815, 44.6%) in the SIATs with neurosurgical level II TCs. Observed versus expected mortality (OE) was not statistically different among the three types of centre with a neurosurgical unit; however, the best mean OE values were observed in the level I TC in the SIAT with no neurosurgical unit.
Conclusion: The Hub and Spoke concept was fully applied in the SIAT in which neurosurgical facilities were available in the level I TC only. The performance of this system suggests that competition among level I and level II TCs in the same Trauma System reduces performance in both. The density of neurosurgical centres must be considered by public health system governors before implementing trauma systems.
Keywords: Trauma management; clinical governance; neurosurgery; quality In health care.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Franco Taggi e Pietro Marturano. “Quanto ci costa il trauma? “Salute e Sicurezza Stradale: l’Onda Lunga del Trauma. C.A.F.I. Editore, Roma: 2007:565–70.
-
- Automobile Club d’Italia, Anno 2013 Incidenti Stradali, novembre 2014. http://www.istat.it/it/archivio/137546ISTAT
-
- ETSC (European Transport Safety Council). Annual PIN Report. 2014. http://etsc.eu/8th-annual-road-safety-performance-index-pin-report/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical