

Oncolytic H-1 Parvovirus Shows Safety and Signs of Immunogenic Activity in a First Phase I/IIa Glioblastoma Trial
- PMID: 28967558
- PMCID: PMC5768665
- DOI: 10.1016/j.ymthe.2017.08.016
Oncolytic H-1 Parvovirus Shows Safety and Signs of Immunogenic Activity in a First Phase I/IIa Glioblastoma Trial
Abstract
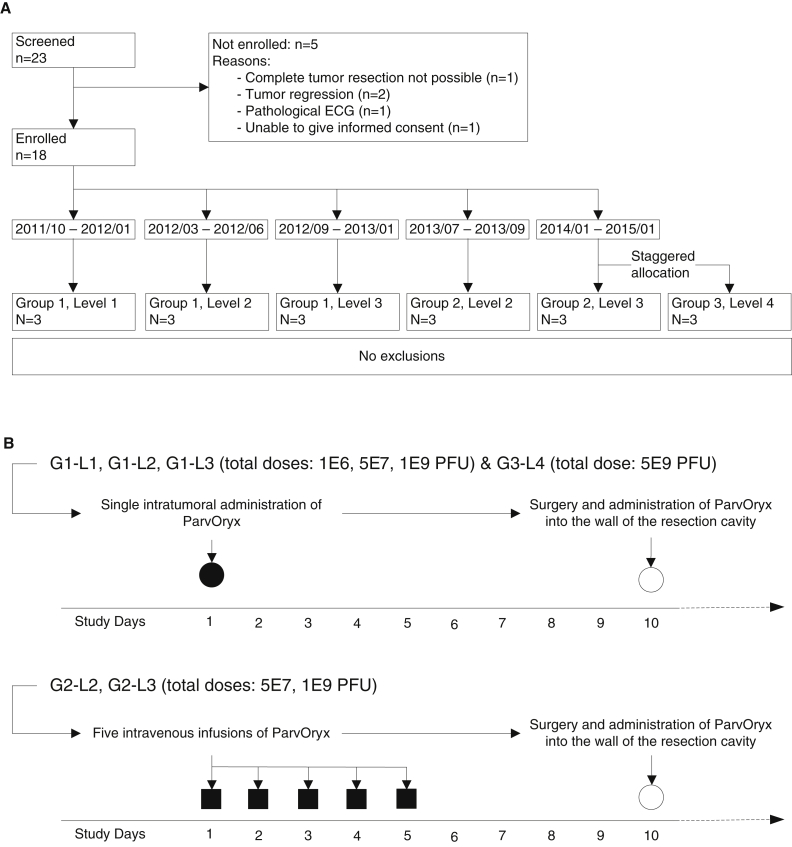
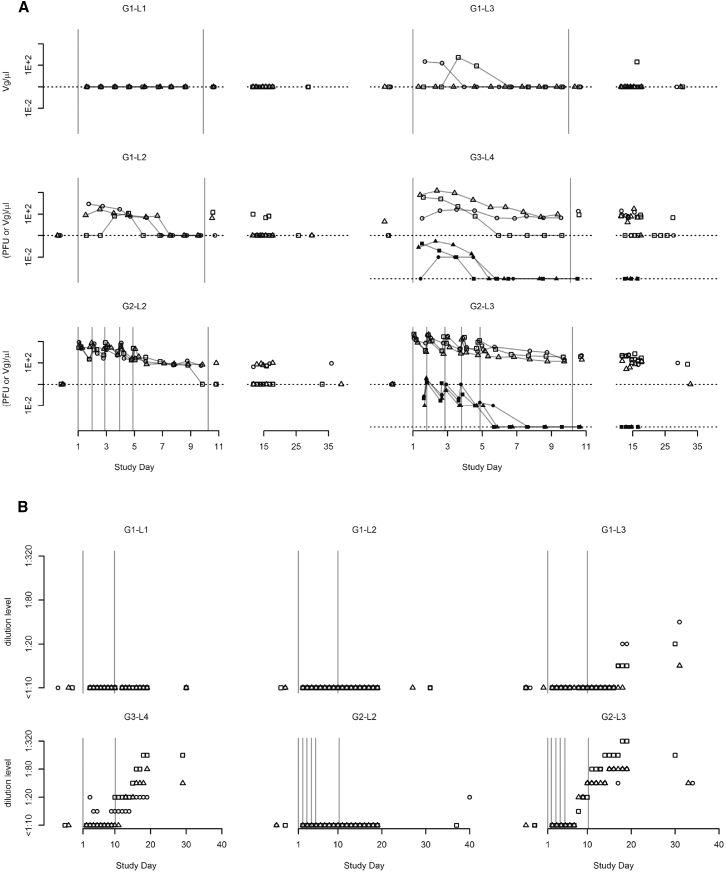
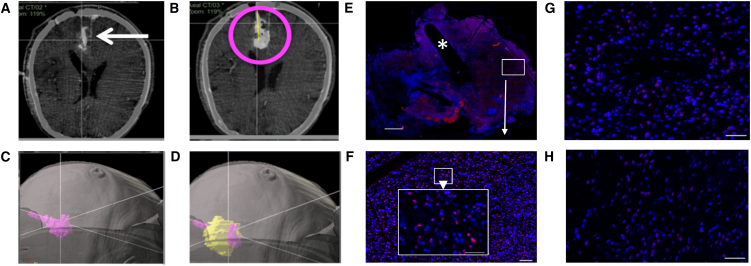
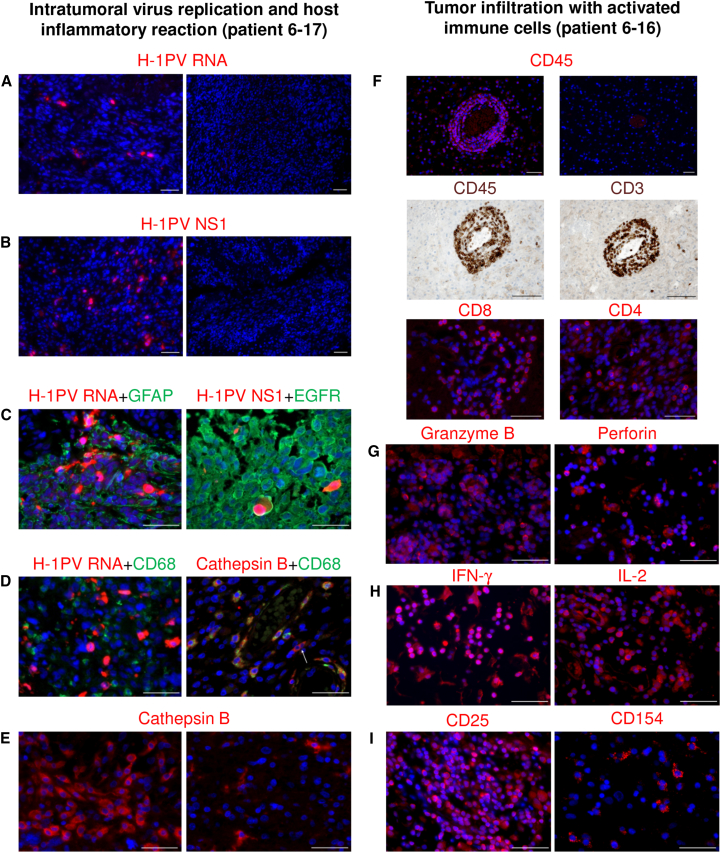
Oncolytic virotherapy may be a means of improving the dismal prognosis of malignant brain tumors. The rat H-1 parvovirus (H-1PV) suppresses tumors in preclinical glioma models, through both direct oncolysis and stimulation of anticancer immune responses. This was the basis of ParvOryx01, the first phase I/IIa clinical trial of an oncolytic parvovirus in recurrent glioblastoma patients. H-1PV (escalating dose) was administered via intratumoral or intravenous injection. Tumors were resected 9 days after treatment, and virus was re-administered around the resection cavity. Primary endpoints were safety and tolerability, virus distribution, and maximum tolerated dose (MTD). Progression-free and overall survival and levels of viral and immunological markers in the tumor and peripheral blood were also investigated. H-1PV treatment was safe and well tolerated, and no MTD was reached. The virus could cross the blood-brain/tumor barrier and spread widely through the tumor. It showed favorable pharmacokinetics, induced antibody formation in a dose-dependent manner, and triggered specific T cell responses. Markers of virus replication, microglia/macrophage activation, and cytotoxic T cell infiltration were detected in infected tumors, suggesting that H-1PV may trigger an immunogenic stimulus. Median survival was extended in comparison with recent meta-analyses. Altogether, ParvOryx01 results provide an impetus for further H-1PV clinical development.
Keywords: clinical trial; glioblastoma; oncolytic parvovirus; tumor microenvironment.
Copyright © 2017 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Stupp R., Hegi M.E., Mason W.P., van den Bent M.J., Taphoorn M.J., Janzer R.C., Ludwin S.K., Allgeier A., Fisher B., Belanger K., European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups. National Cancer Institute of Canada Clinical Trials Group Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
-
- Clarke J.L., Ennis M.M., Yung W.K., Chang S.M., Wen P.Y., Cloughesy T.F., Deangelis L.M., Robins H.I., Lieberman F.S., Fine H.A., North American Brain Tumor Consortium Is surgery at progression a prognostic marker for improved 6-month progression-free survival or overall survival for patients with recurrent glioblastoma? Neuro-oncol. 2011;13:1118–1124. - PMC - PubMed
-
- Lichty B.D., Breitbach C.J., Stojdl D.F., Bell J.C. Going viral with cancer immunotherapy. Nat. Rev. Cancer. 2014;14:559–567. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
