

A longitudinal study of the infant nasopharyngeal microbiota: The effects of age, illness and antibiotic use in a cohort of South East Asian children
- PMID: 28968382
- PMCID: PMC5638608
- DOI: 10.1371/journal.pntd.0005975
A longitudinal study of the infant nasopharyngeal microbiota: The effects of age, illness and antibiotic use in a cohort of South East Asian children
Abstract
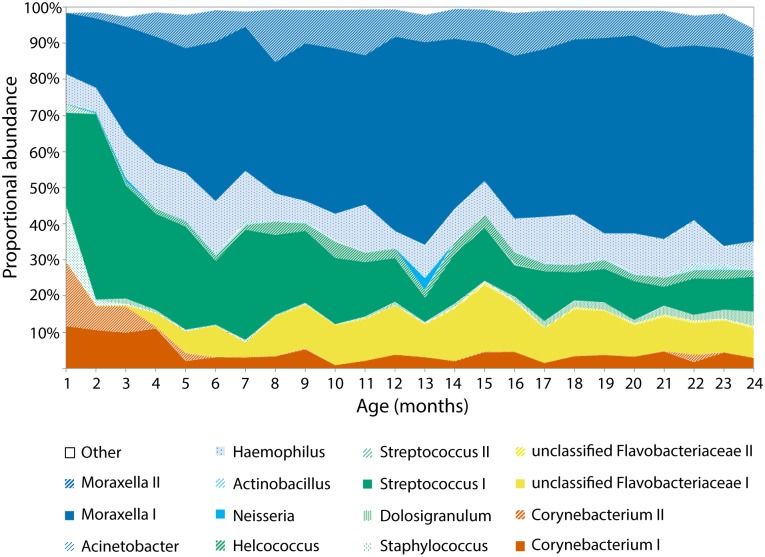
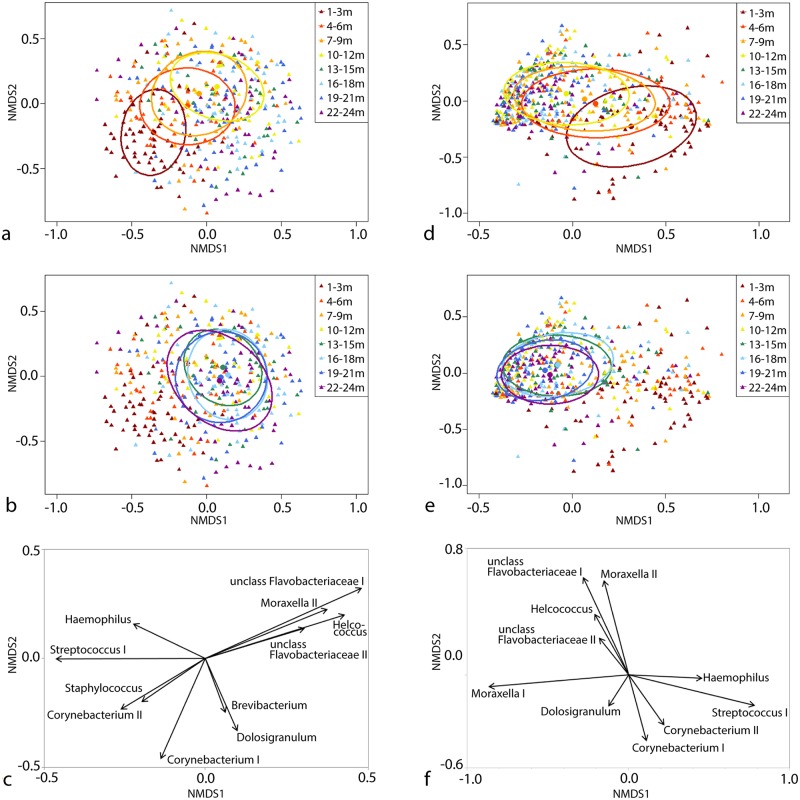
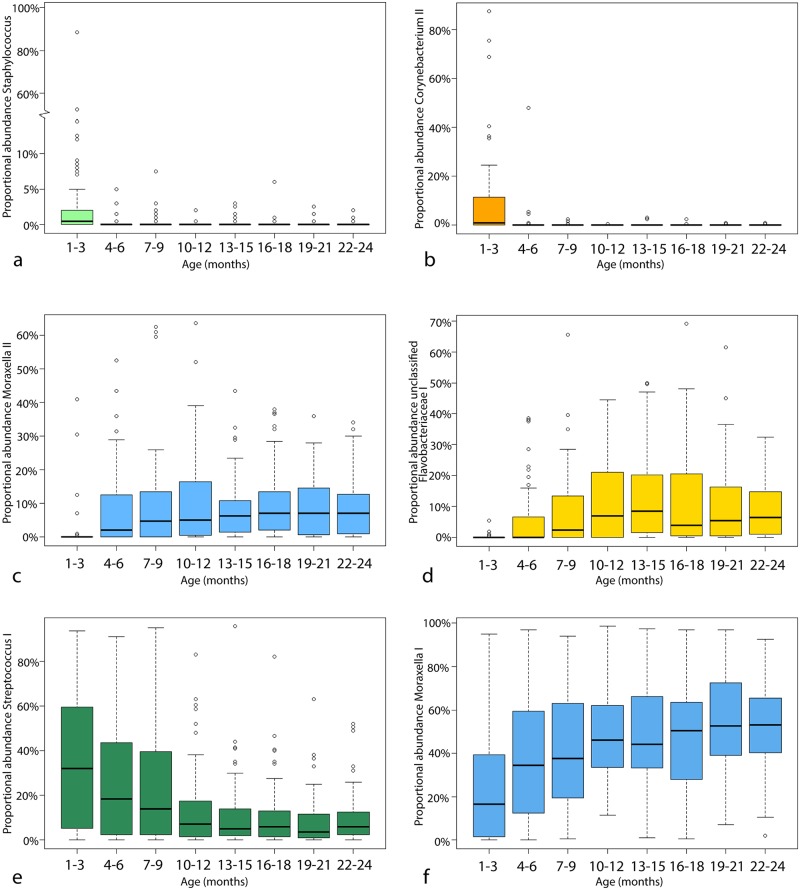
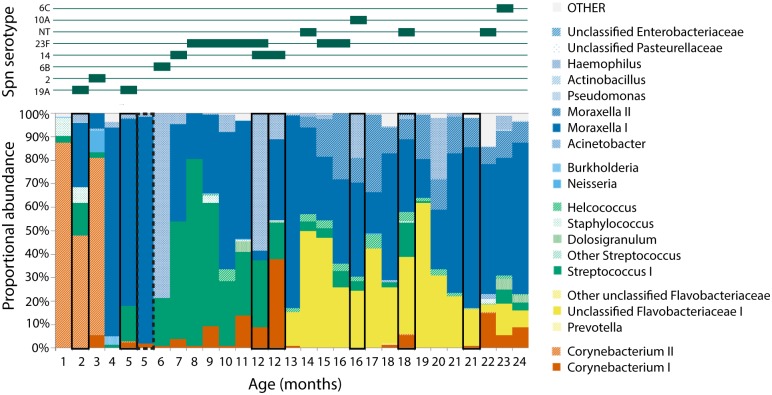
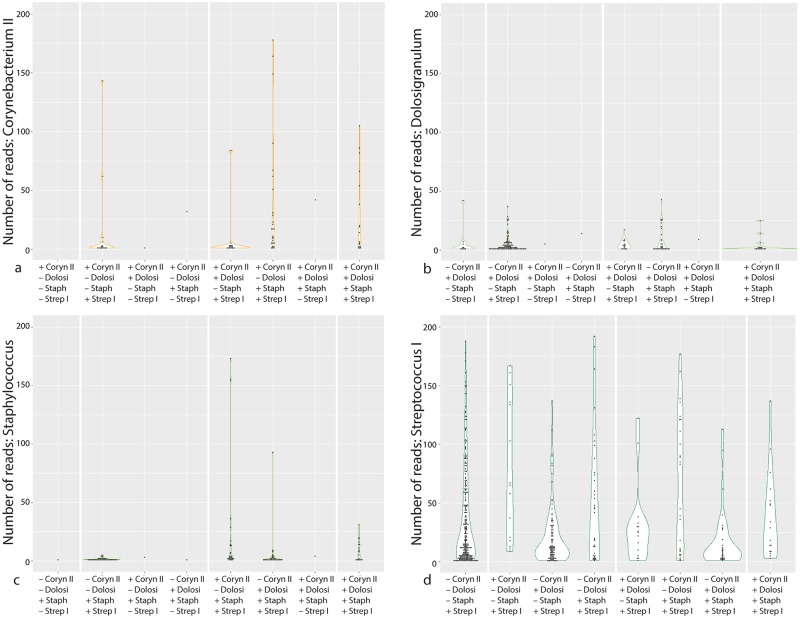
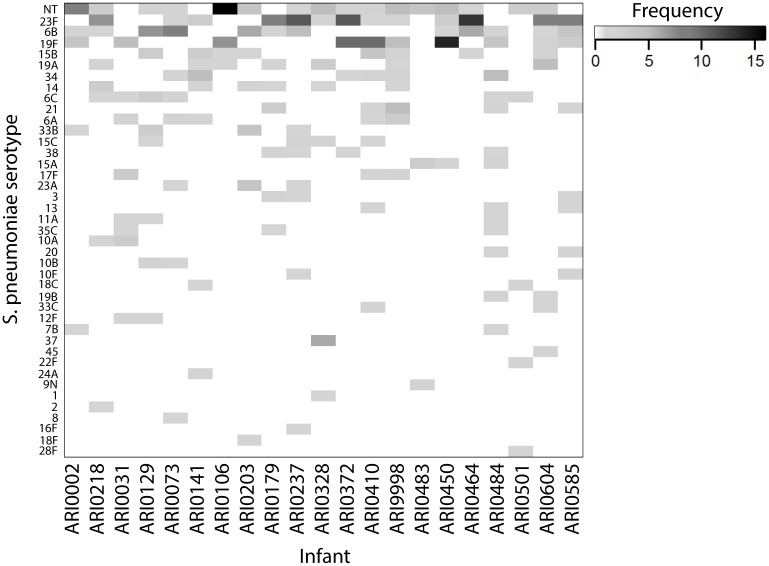
A longitudinal study was undertaken in infants living in the Maela refugee camp on the Thailand-Myanmar border between 2007 and 2010. Nasopharyngeal swabs were collected monthly, from birth to 24 months of age, with additional swabs taken if the infant was diagnosed with pneumonia according to WHO clinical criteria. At the time of collection, swabs were cultured for Streptococcus pneumoniae and multiple serotype carriage was assessed. The bacterial 16S rRNA gene profiles of 544 swabs from 21 infants were analysed to see how the microbiota changes with age, respiratory infection, antibiotic consumption and pneumococcal acquisition. The nasopharyngeal microbiota is a somewhat homogenous community compared to that of other body sites. In this cohort it is dominated by five taxa: Moraxella, Streptococcus, Haemophilus, Corynebacterium and an uncharacterized Flavobacteriaceae taxon of 93% nucleotide similarity to Ornithobacterium. Infant age correlates with certain changes in the microbiota across the cohort: Staphylococcus and Corynebacterium are associated with the first few months of life while Moraxella and the uncharacterised Flavobacteriaceae increase in proportional abundance with age. Respiratory illness and antibiotic use often coincide with an unpredictable perturbation of the microbiota that differs from infant to infant and in different illness episodes. The previously described interaction between Dolosigranulum and Streptococcus was observed in these data. Monthly sampling demonstrates that the nasopharyngeal microbiota is in flux throughout the first two years of life, and that in this refugee camp population the pool of potential bacterial colonisers may be limited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Succession and determinants of the early life nasopharyngeal microbiota in a South African birth cohort.Microbiome. 2023 Jun 5;11(1):127. doi: 10.1186/s40168-023-01563-5. Microbiome. 2023. PMID: 37271810 Free PMC article.
-
The association between pneumococcal vaccination, ethnicity, and the nasopharyngeal microbiota of children in Fiji.Microbiome. 2019 Jul 16;7(1):106. doi: 10.1186/s40168-019-0716-4. Microbiome. 2019. PMID: 31311598 Free PMC article. Clinical Trial.
-
Development of the Nasopharyngeal Microbiota in Infants with Cystic Fibrosis.Am J Respir Crit Care Med. 2016 Mar 1;193(5):504-15. doi: 10.1164/rccm.201509-1759OC. Am J Respir Crit Care Med. 2016. PMID: 26492486
-
Report from a WHO Working Group: standard method for detecting upper respiratory carriage of Streptococcus pneumoniae.Pediatr Infect Dis J. 2003 Feb;22(2):e1-11. doi: 10.1097/01.inf.0000049347.42983.77. Pediatr Infect Dis J. 2003. PMID: 12586987 Review.
-
Microbiota succession throughout life from the cradle to the grave.Nat Rev Microbiol. 2022 Dec;20(12):707-720. doi: 10.1038/s41579-022-00768-z. Epub 2022 Jul 29. Nat Rev Microbiol. 2022. PMID: 35906422 Review.
Cited by
-
Exploring the pediatric nasopharyngeal bacterial microbiota with culture-based MALDI-TOF mass spectrometry and targeted metagenomic sequencing.mBio. 2024 Jun 12;15(6):e0078424. doi: 10.1128/mbio.00784-24. Epub 2024 Apr 29. mBio. 2024. PMID: 38682956 Free PMC article.
-
Succession and determinants of the early life nasopharyngeal microbiota in a South African birth cohort.Microbiome. 2023 Jun 5;11(1):127. doi: 10.1186/s40168-023-01563-5. Microbiome. 2023. PMID: 37271810 Free PMC article.
-
Infant Nasopharyngeal Microbiota Subphenotypes and Early Childhood Lung Function: Evidence from a Rural Ghanaian Pregnancy Cohort.Int J Environ Res Public Health. 2021 Jul 7;18(14):7276. doi: 10.3390/ijerph18147276. Int J Environ Res Public Health. 2021. PMID: 34299726 Free PMC article.
-
RSV Infection in Refugees and Asylum Seekers: A Systematic Review and Meta-Analysis.Epidemiologia (Basel). 2024 May 27;5(2):221-249. doi: 10.3390/epidemiologia5020016. Epidemiologia (Basel). 2024. PMID: 38920751 Free PMC article. Review.
-
The nasopharyngeal microbiota in patients with viral respiratory tract infections is enriched in bacterial pathogens.Eur J Clin Microbiol Infect Dis. 2018 Sep;37(9):1725-1733. doi: 10.1007/s10096-018-3305-8. Epub 2018 Jul 22. Eur J Clin Microbiol Infect Dis. 2018. PMID: 30033505
References
-
- Kinabo GD, van der Ven A, Msuya LJ, Shayo AM, Schimana W, Ndaro A, et al. Dynamics of nasopharyngeal bacterial colonisation in HIV-exposed young infants in Tanzania. Tropical Medicine and International Health. 2013;18(3):286–95. doi: 10.1111/tmi.12057 - DOI - PubMed
-
- Stearns JC, Davidson CJ, McKeon S, Whelan FJ, Fontes ME, Schryvers AB, et al. Culture and molecular-based profiles show shifts in bacterial communities of the upper respiratory tract that occur with age. ISME Journal. 2015;9(5):1246–59. doi: 10.1038/ismej.2014.250 - DOI - PMC - PubMed
-
- Garenne M, Ronsmans C, Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Statistic Quarterly. 1992;45:180–91. - PubMed
-
- Langdon A, Crook N, Dantas G. The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Medicine. 2016;8:39 doi: 10.1186/s13073-016-0294-z - DOI - PMC - PubMed
-
- Suárez-Arrabal MC, Mella C, Lopez SM, Brown NV, Hall MW, Hammond S, et al. Nasopharyngeal bacterial burden and antibiotics: Influence on inflammatory markers and disease severity in infants with respiratory syncytial virus bronchiolitis. The Journal of Infection. 2015;71(4):458–69. doi: 10.1016/j.jinf.2015.06.010 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
