

Loss of long-term non-progressor and HIV controller status over time in the French Hospital Database on HIV - ANRS CO4
- PMID: 28968404
- PMCID: PMC5624574
- DOI: 10.1371/journal.pone.0184441
Loss of long-term non-progressor and HIV controller status over time in the French Hospital Database on HIV - ANRS CO4
Abstract
Objectives: We studied the frequency and risk factors for loss of long-term non-progressor (LTNP) and HIV controller (HIC) status among patients identified as such in 2005 in the French Hospital Database on HIV (FHDH-ANRS CO4).
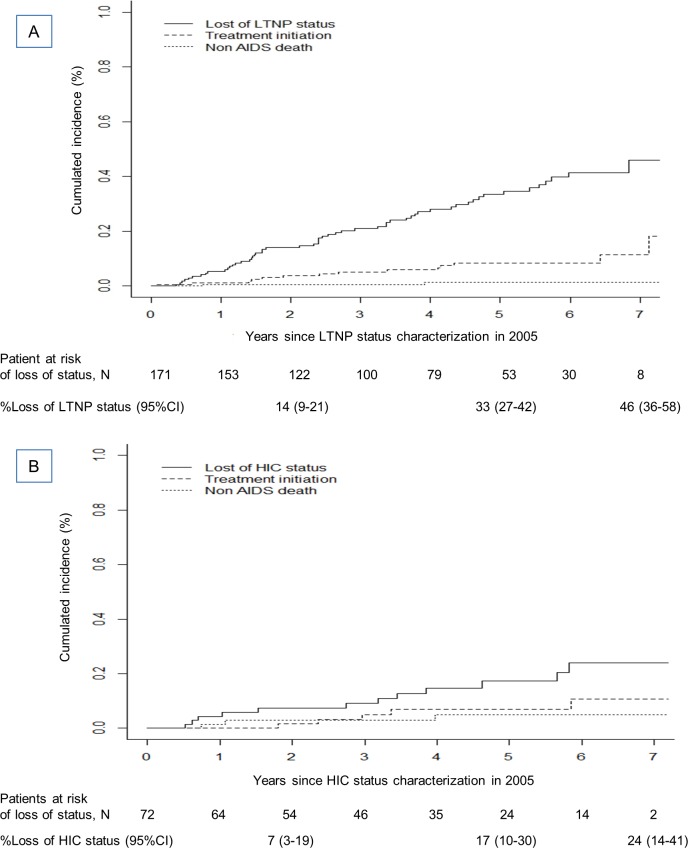
Methods: We selected patients who were treatment-naïve and asymptomatic in 2005 (baseline). Those with ≥8 years of known HIV infection and a CD4 cell nadir ≥500/mm3 were classified as LTNP and those with ≥10 years of known HIV infection and 90% of plasma viral load (VL) values ≤500 copies/ml in the absence of cART as HIC. cART initiation without loss of status and death from non AIDS-defining causes were considered as competing events.
Results: After 5 years of follow-up, 33% (95%CI; 27-42) of 171 LTNP patients and 17% (95%CI; 10-30) of 72 HIC patients had lost their status. In multivariable analyses, loss of LTNP status was associated with lower baseline CD4 cell counts and CD4/CD8 ratios. Only VL was significantly associated with loss of HIC status after adjustment for the baseline CD4 cell count, the CD4/CD8 ratio, and concomitant LTNP status. The hazard ratio for loss of HIC status was 5.5 (95%CI, 1.5-20.1) for baseline VL 50-500 vs ≤50 cp/mL, after adjustment for the baseline CD4 cell count.
Conclusions: One-third of LTNP and one-fifth of HIC patients lost their status after 5 years of follow-up, raising questions as to the possible benefits and timing of ART initiation in these populations.
Conflict of interest statement
Figures
Similar articles
-
Prevalence and comparative characteristics of long-term nonprogressors and HIV controller patients in the French Hospital Database on HIV.AIDS. 2009 Jun 1;23(9):1163-9. doi: 10.1097/QAD.0b013e32832b44c8. AIDS. 2009. PMID: 19444075
-
CD4+/CD8+ ratio restoration in long-term treated HIV-1-infected individuals.AIDS. 2017 Jul 31;31(12):1685-1695. doi: 10.1097/QAD.0000000000001533. AIDS. 2017. PMID: 28700392
-
Early control of HIV-1 infection in long-term nonprogressors followed since diagnosis in the ANRS SEROCO/HEMOCO cohort.J Acquir Immune Defic Syndr. 2009 Jan 1;50(1):19-26. doi: 10.1097/QAI.0b013e31818ce709. J Acquir Immune Defic Syndr. 2009. PMID: 19295331
-
[National consensus document by GESIDA/National Aids Plan on antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2011 update)].Enferm Infecc Microbiol Clin. 2011 Mar;29(3):209.e1-103. doi: 10.1016/j.eimc.2010.12.004. Enferm Infecc Microbiol Clin. 2011. PMID: 21388714 Spanish.
-
[Consensus document of Gesida and Spanish Secretariat for the National Plan on AIDS (SPNS) regarding combined antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2012)].Enferm Infecc Microbiol Clin. 2012 Jun;30(6):e1-89. doi: 10.1016/j.eimc.2012.03.006. Epub 2012 May 23. Enferm Infecc Microbiol Clin. 2012. PMID: 22633764 Spanish.
Cited by
-
How Unavoidable Are Analytical Treatment Interruptions in HIV Cure-Related Studies?J Infect Dis. 2019 Jul 2;220(220 Suppl 1):S24-S26. doi: 10.1093/infdis/jiz222. J Infect Dis. 2019. PMID: 31264691 Free PMC article.
-
HIV control: Is getting there the same as staying there?PLoS Pathog. 2018 Nov 1;14(11):e1007222. doi: 10.1371/journal.ppat.1007222. eCollection 2018 Nov. PLoS Pathog. 2018. PMID: 30383857 Free PMC article. Review.
-
Naïve CD4+ cell counts significantly decay and high HIV RNA levels contribute to immunological progression in long-term non-progressors infected with HIV by blood products: a cohort study.BMC Immunol. 2021 Jun 3;22(1):36. doi: 10.1186/s12865-021-00426-8. BMC Immunol. 2021. PMID: 34082709 Free PMC article.
-
A case of human immunodeficiency virus (HIV) infection without increase in HIV RNA level: A rare observation during the modern antiretroviral therapy era.J Gen Fam Med. 2021 Aug 23;23(2):101-103. doi: 10.1002/jgf2.492. eCollection 2022 Mar. J Gen Fam Med. 2021. PMID: 35261857 Free PMC article.
-
Elite controllers: A heterogeneous group of HIV-infected patients.Virulence. 2020 Dec;11(1):889-897. doi: 10.1080/21505594.2020.1788887. Virulence. 2020. PMID: 32698654 Free PMC article. Review.
References
-
- Gurdasani D, Iles L, Dillon DG, Young EH, Olson AD, Naranbhai V, et al. A systematic review of definitions of extreme phenotypes of HIV control and progression. AIDS 2014; 28(2):149–162. doi: 10.1097/QAD.0000000000000049 - DOI - PMC - PubMed
-
- Madec Y, Boufassa F, Porter K, Prins M, Sabin C, d'Arminio Monforte A, et al. Natural history of HIV-control since seroconversion. AIDS 2013; 27(15):2451–2460. doi: 10.1097/01.aids.0000431945.72365.01 - DOI - PubMed
-
- Noel N, Lerolle N, Lecuroux C, Goujard C, Venet A, Saez-Cirion A, et al. Immunologic and Virologic Progression in HIV Controllers: The Role of Viral "Blips" and Immune Activation in the ANRS CO21 CODEX Study. PLoS One 2015; 10(7):e0131922 doi: 10.1371/journal.pone.0131922 - DOI - PMC - PubMed
-
- Leon A, Perez I, Ruiz-Mateos E, Benito JM, Leal M, Lopez-Galindez C, et al. Rate and predictors of progression in elite and viremic HIV-1 controllers. AIDS 2016; 30(8):1209–1220. doi: 10.1097/QAD.0000000000001050 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
