

High-grade glioma in very young children: a rare and particular patient population
- PMID: 28969094
- PMCID: PMC5610026
- DOI: 10.18632/oncotarget.18478
High-grade glioma in very young children: a rare and particular patient population
Abstract
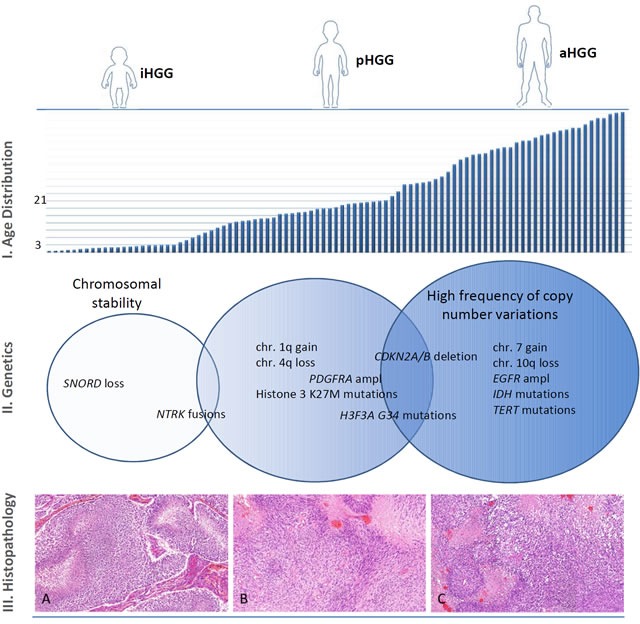
In the past years, pediatric high-grade gliomas (HGG) have been the focus of several research articles and reviews, given the recent discoveries on the genetic and molecular levels pointing out a clinico-biological uniqueness of the pediatric population compared to their adult counterparts with HGG. On the other hand, there are only scarce data about HGG in very young children (below 3 years of age at diagnosis) due to their relatively low incidence. However, the few available data suggest further distinction of this very rare subgroup from older children and adults at several levels including their molecular and biological characteristics, their treatment management, as well as their outcome. This review summarizes and discusses the current available knowledge on the epidemiological, neuropathological, genetic and molecular data of this subpopulation. We discuss these findings and differences compared to older patients suffering from the same histologic disease. In addition, we highlight the particular clinical and neuro-radiological findings in this specific subgroup of patients as well as their current management approaches and treatment outcomes.
Keywords: brain tumors; chemotherapy; high-grade glioma; infants; radiotherapy.
Conflict of interest statement
CONFLICTS OF INTEREST There is no conflict of interest.
Figures
References
-
- Ostrom QT, De Blank PM, Kruchko C, Petersen CM, Liao P, Finlay JL, Stearns DS, Wolff JE, Wolinsky Y, Letterio JJ, Barnholtz-Sloan JS. Alex's Lemonade stand foundation infant and childhood primary brain and central nervous system tumors diagnosed in the United States in 2007-2011. Neuro Oncol. 2015;16:x1–35. doi: 10.1093/neuonc/nou327. - DOI - PMC - PubMed
-
- Broniscer A, Gajjar A. Supratentorial high-grade astrocytoma and diffuse brainstem glioma: two challenges for the pediatric oncologist. Oncologist. 2004;9:197–206. - PubMed
-
- Cohen KJ, Pollack IF, Zhou T, Buxton A, Holmes EJ, Burger PC, Brat DJ, Rosenblum MK, Hamilton RL, Lavey RS, Heideman RL. Temozolomide in the treatment of high-grade gliomas in children: A report from the Children's Oncology Group. Neuro Oncol. 2011;13:317–23. doi: 10.1093/neuonc/noq191. - DOI - PMC - PubMed
-
- Jones C, Karajannis MA, Jones DTW, Kieran MW, Monje M, Baker SJ, Becher OJ, Cho YJ, Gupta N, Hawkins C, Hargrave D, Haas-Kogan DA, Jabado N, et al. Pediatric high-grade glioma: biologically and clinically in need of new thinking. Neuro Oncol. 2017;9:153–161. doi: 10.1093/neuonc/now101. - DOI - PMC - PubMed
-
- Dufour C, Grill J, Lellouch-Tubiana A, Puget S, Chastagner P, Frappaz D, Doz F, Pichon F, Plantaz D, Gentet JC, Raquin MA, Kalifa C. High-grade glioma in children under 5 years of age: A chemotherapy only approach with the BBSFOP protocol. Eur J Cancer. 2006;42:2939–45. doi: 10.1016/j.ejca.2006.06.021. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
