

A Transdiagnostic Review of Negative Symptom Phenomenology and Etiology
- PMID: 28969356
- PMCID: PMC5472109
- DOI: 10.1093/schbul/sbx066
A Transdiagnostic Review of Negative Symptom Phenomenology and Etiology
Abstract
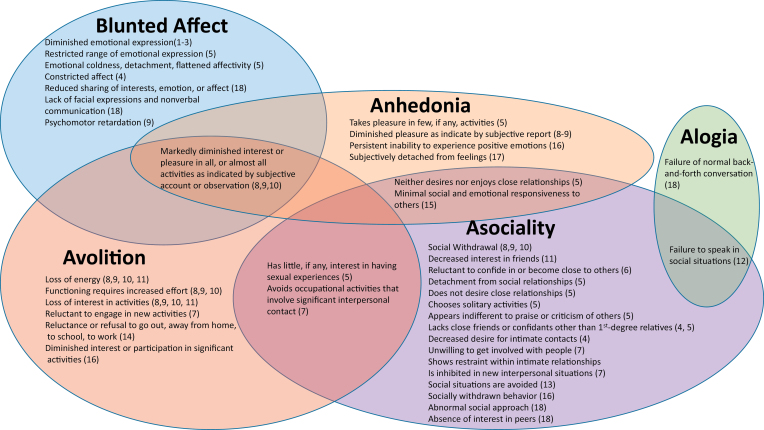
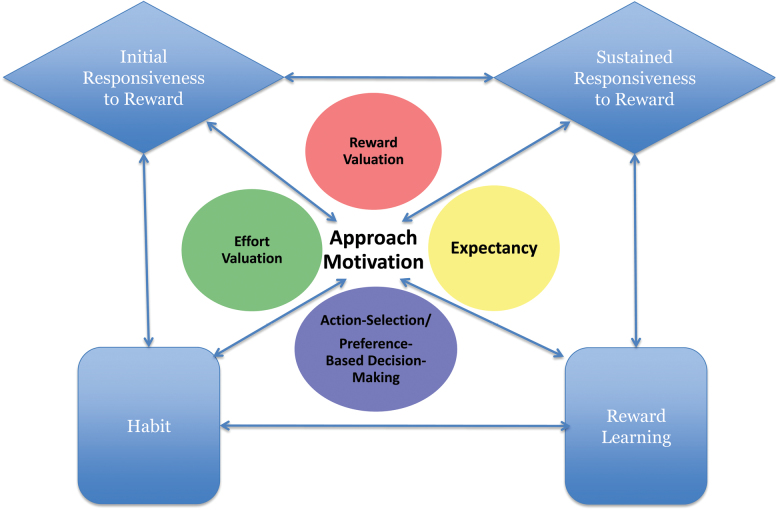
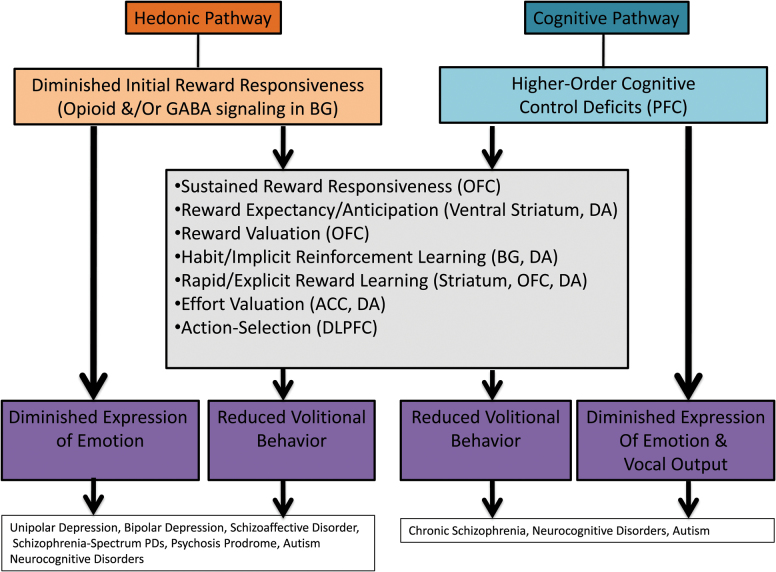
In the DSM5, negative symptoms are 1 of the 5 core dimensions of psychopathology evaluated for schizophrenia. However, negative symptoms are not pathognomonic-they are also part of the diagnostic criteria for other schizophrenia-spectrum disorders, disorders that sometimes have comorbid psychosis, diagnoses not in the schizophrenia-spectrum, and the general "nonclinical" population. Although etiological models of negative symptoms have been developed for chronic schizophrenia, there has been little attention given to whether these models have transdiagnostic applicability. In the current review, we examine areas of commonality and divergence in the clinical presentation and etiology of negative symptoms across diagnostic categories. It was concluded that negative symptoms are relatively frequent across diagnostic categories, but individual disorders may differ in whether their negative symptoms are persistent/transient or primary/secondary. Evidence for separate dimensions of volitional and expressive symptoms exists, and there may be multiple mechanistic pathways to the same symptom phenomenon among DSM-5 disorders within and outside the schizophrenia-spectrum (ie, equifinality). Evidence for a novel transdiagnostic etiological model is presented based on the Research Domain Criteria (RDoC) constructs, which proposes the existence of 2 such pathways-a hedonic pathway and a cognitive pathway-that can both lead to expressive or volitional symptoms. To facilitate treatment breakthroughs, future transdiagnostic studies on negative symptoms are warranted that explore mechanisms underlying volitional and expressive pathology.
Keywords: alogia; anhedonia; asociality; avolition; blunted affect.
© The Author 2017. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Bleuler E. Dementia praecox or the group of schizophrenias. Vertex. 2010;21:394–400. - PubMed
-
- Kraepelin E. Dementia Praecox and Paraphrenia (Barclay R. M., Trans.). New York, NY: Krieger; 1919.
-
- Peralta V, Cuesta MJ. How many and which are the psychopathological dimensions in schizophrenia? Issues influencing their ascertainment. Schizophr Res. 2001;49:269–285. - PubMed
-
- Fervaha G, Remington G. Validation of an abbreviated quality of life scale for schizophrenia. Eur Neuropsychopharmacol. 2013;23:1072–1077. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
