

Glymphatic MRI in idiopathic normal pressure hydrocephalus
- PMID: 28969373
- PMCID: PMC5841149
- DOI: 10.1093/brain/awx191
Glymphatic MRI in idiopathic normal pressure hydrocephalus
Abstract
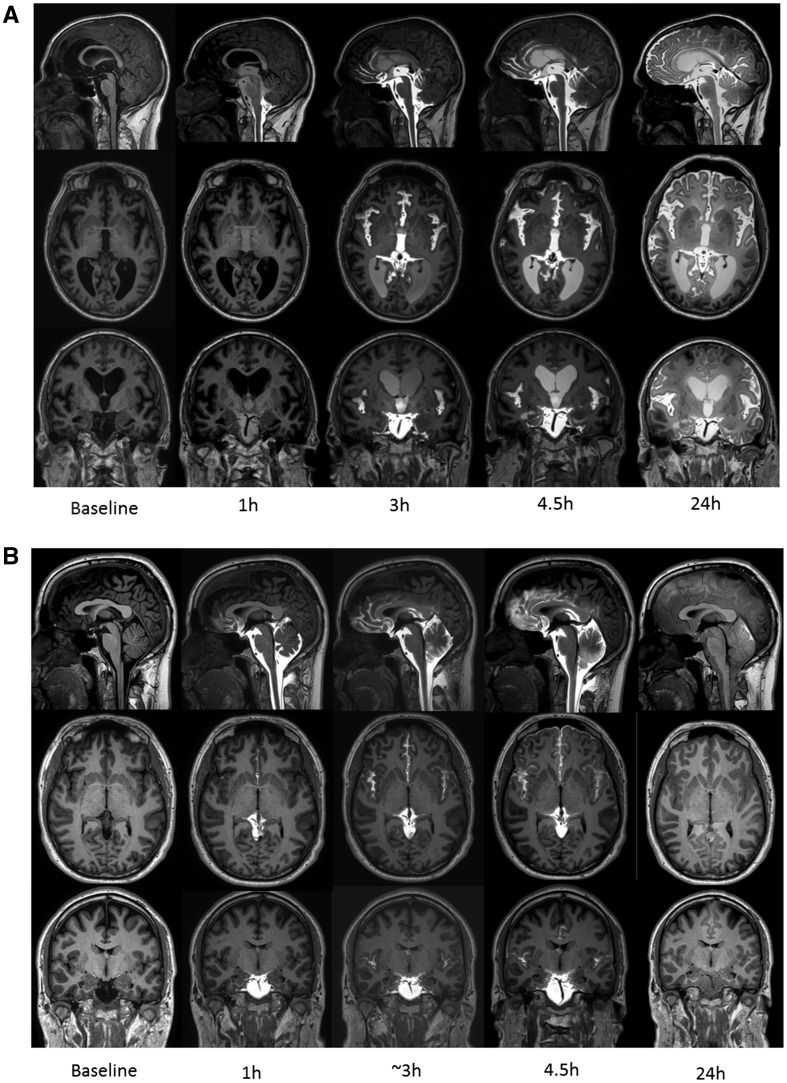
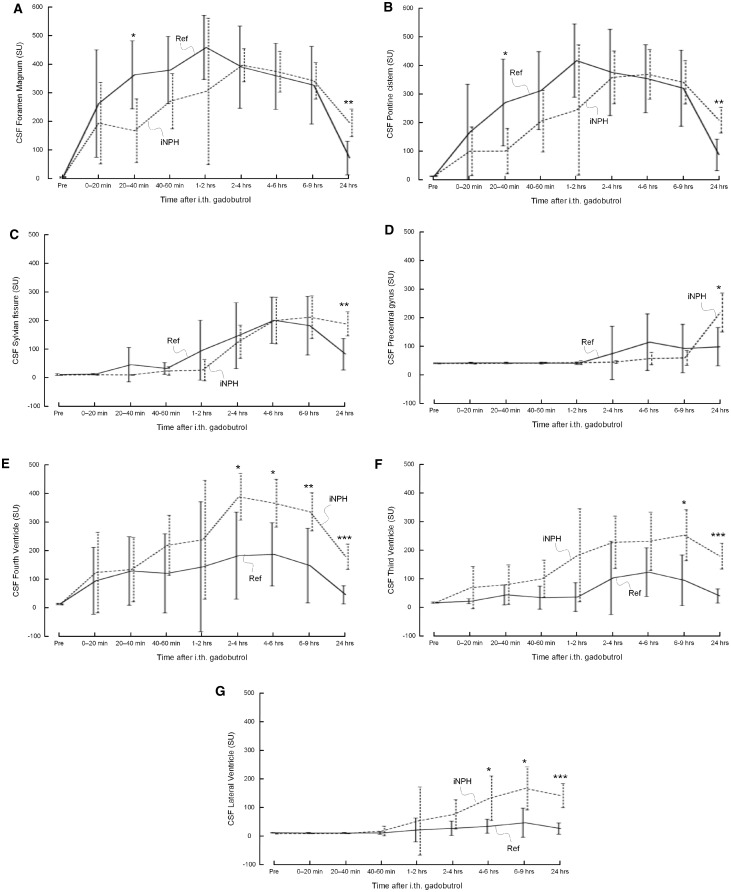
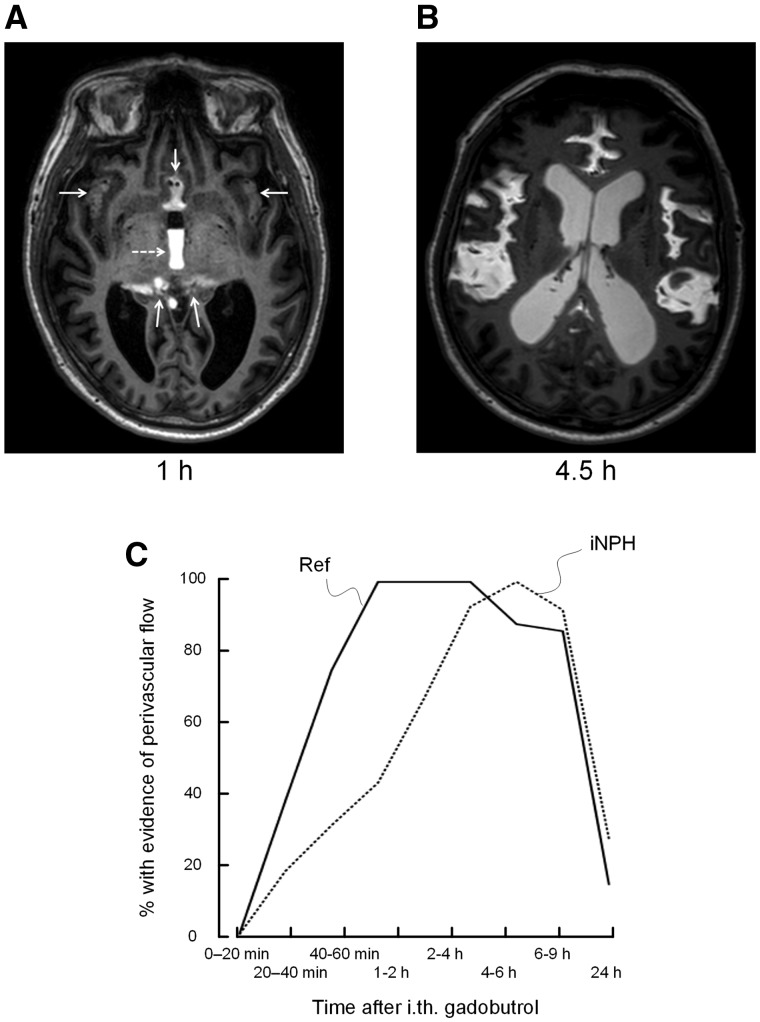
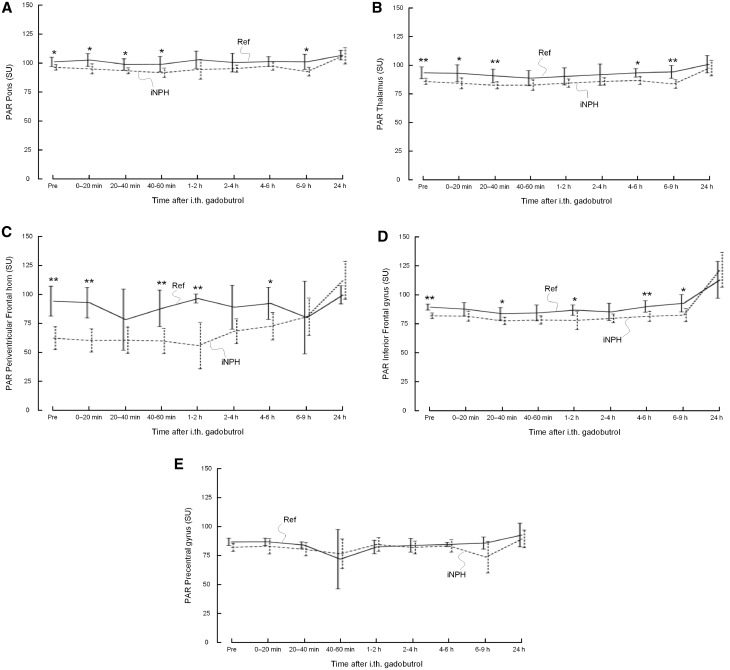
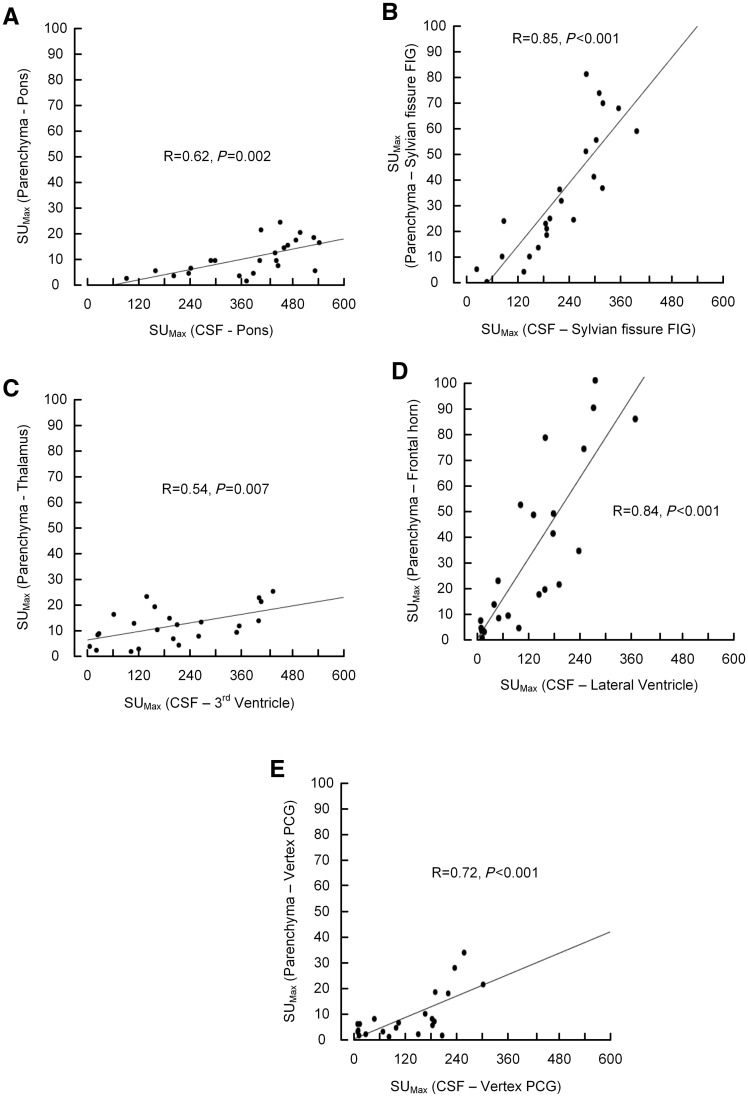
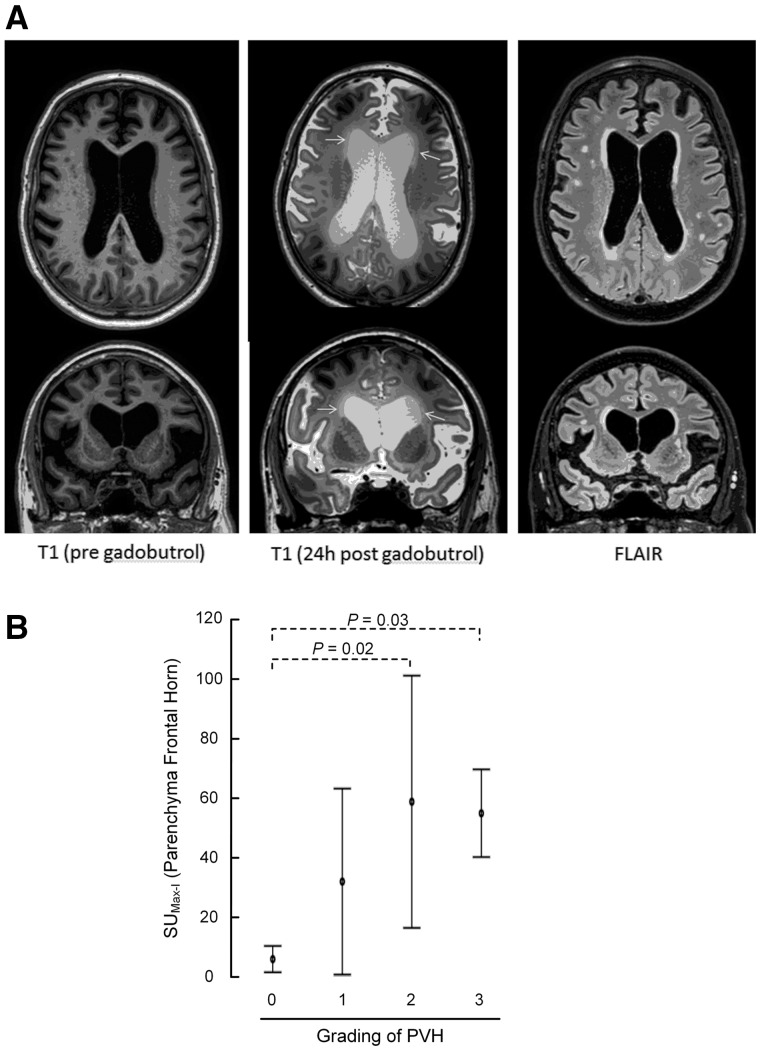
The glymphatic system has in previous studies been shown as fundamental to clearance of waste metabolites from the brain interstitial space, and is proposed to be instrumental in normal ageing and brain pathology such as Alzheimer's disease and brain trauma. Assessment of glymphatic function using magnetic resonance imaging with intrathecal contrast agent as a cerebrospinal fluid tracer has so far been limited to rodents. We aimed to image cerebrospinal fluid flow characteristics and glymphatic function in humans, and applied the methodology in a prospective study of 15 idiopathic normal pressure hydrocephalus patients (mean age 71.3 ± 8.1 years, three female and 12 male) and eight reference subjects (mean age 41.1 + 13.0 years, six female and two male) with suspected cerebrospinal fluid leakage (seven) and intracranial cyst (one). The imaging protocol included T1-weighted magnetic resonance imaging with equal sequence parameters before and at multiple time points through 24 h after intrathecal injection of the contrast agent gadobutrol at the lumbar level. All study subjects were kept in the supine position between examinations during the first day. Gadobutrol enhancement was measured at all imaging time points from regions of interest placed at predefined locations in brain parenchyma, the subarachnoid and intraventricular space, and inside the sagittal sinus. Parameters demonstrating gadobutrol enhancement and clearance in different locations were compared between idiopathic normal pressure hydrocephalus and reference subjects. A characteristic flow pattern in idiopathic normal hydrocephalus was ventricular reflux of gadobutrol from the subarachnoid space followed by transependymal gadobutrol migration. At the brain surfaces, gadobutrol propagated antegradely along large leptomeningeal arteries in all study subjects, and preceded glymphatic enhancement in adjacent brain tissue, indicating a pivotal role of intracranial pulsations for glymphatic function. In idiopathic normal pressure hydrocephalus, we found delayed enhancement (P < 0.05) and decreased clearance of gadobutrol (P < 0.05) at the Sylvian fissure. Parenchymal (glymphatic) enhancement peaked overnight in both study groups, possibly indicating a crucial role of sleep, and was larger in normal pressure hydrocephalus patients (P < 0.05 at inferior frontal gyrus). We interpret decreased gadobutrol clearance from the subarachnoid space, along with persisting enhancement in brain parenchyma, as signs of reduced glymphatic clearance in idiopathic normal hydrocephalus, and hypothesize that reduced glymphatic function is instrumental for dementia in this disease. The study shows promise for glymphatic magnetic resonance imaging as a method to assess human brain metabolic function and renders a potential for contrast enhanced brain extravascular space imaging.
Keywords: MRI; cerebrospinal fluid; gadobutrol; glymphatic function; idiopathic normal pressure hydrocephalus.
© The Author (2017). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Comment in
-
Gadobutrol and the End of the Tap Test.World Neurosurg. 2018 Feb;110:442. doi: 10.1016/j.wneu.2017.12.101. Epub 2017 Dec 21. World Neurosurg. 2018. PMID: 29275054 No abstract available.
References
-
- Adams RD, Fisher CM, Hakim S, Ojemann RG, Sweet WH. Symptomatic occult hydrocephalus with "Normal" cerebrospinal-fluid pressure. A treatable syndrome. N Eng J Med 1965; 273: 117–26. - PubMed
-
- Aydin K, Guven K, Sencer S, Jinkins JR, Minareci O. MRI cisternography with gadolinium-containing contrast medium: its role, advantages and limitations in the investigation of rhinorrhoea. Neuroradiology 2004; 46: 75–80. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
