

The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis
- PMID: 28969441
- PMCID: PMC5794524
- DOI: 10.1176/appi.ajp.2017.17040472
The Effect of a Single Dose of Intravenous Ketamine on Suicidal Ideation: A Systematic Review and Individual Participant Data Meta-Analysis
Abstract
Objective: Suicide is a public health crisis with limited treatment options. The authors conducted a systematic review and individual participant data meta-analysis examining the effects of a single dose of ketamine on suicidal ideation.
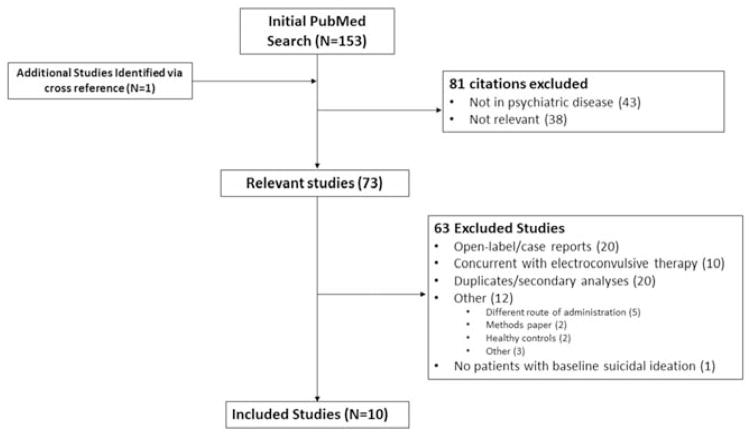
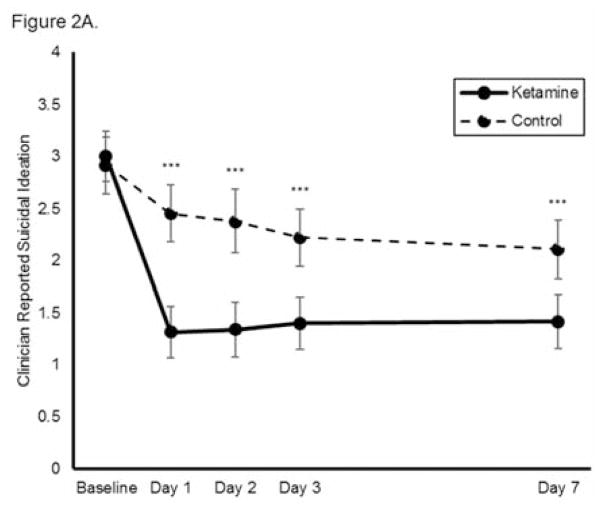
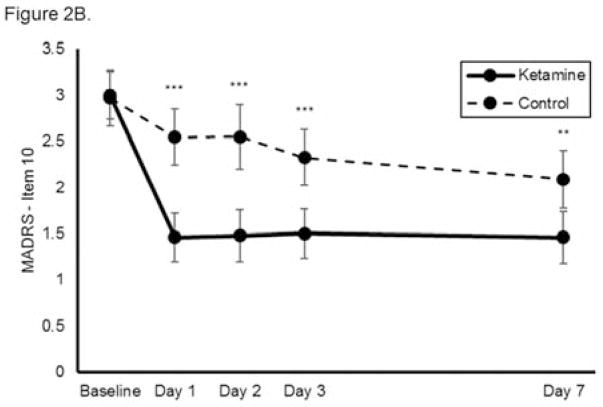
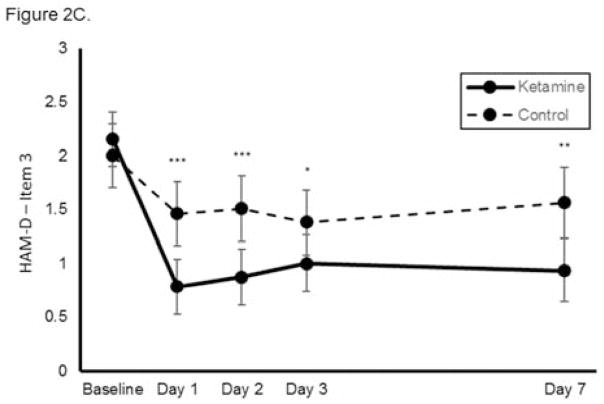
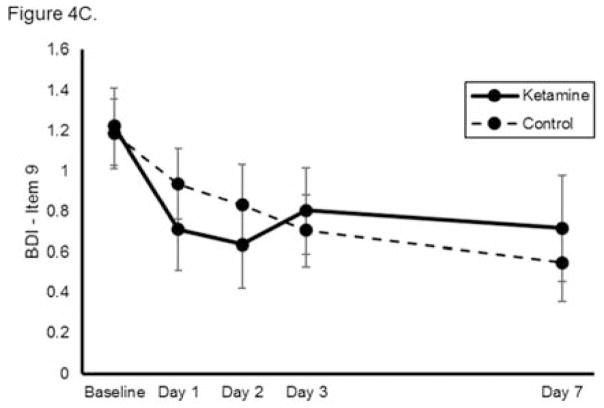
Method: Individual participant data were obtained from 10 of 11 identified comparison intervention studies that used either saline or midazolam as a control treatment. The analysis included only participants who had suicidal ideation at baseline (N=167). A one-stage, individual participant data, meta-analytic procedure was employed using a mixed-effects, multilevel, general linear model. The primary outcome measures were the suicide items from clinician-administered (the Montgomery-Åsberg Depression Rating Scale [MADRS] or the Hamilton Depression Rating Scale [HAM-D]) and self-report scales (the Quick Inventory of Depressive Symptomatology-Self Report [QIDS-SR] or the Beck Depression Inventory [BDI]), obtained for up to 1 week after ketamine administration.
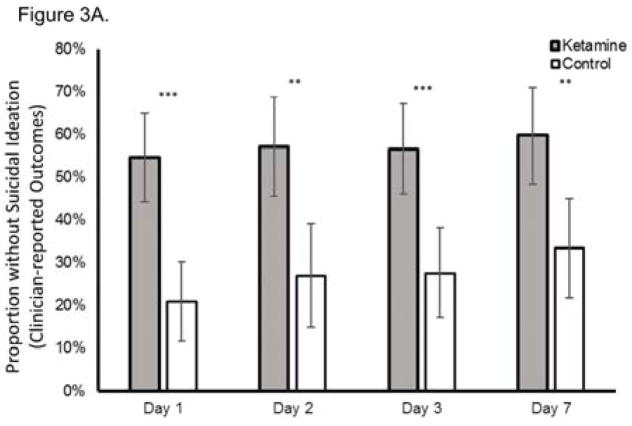
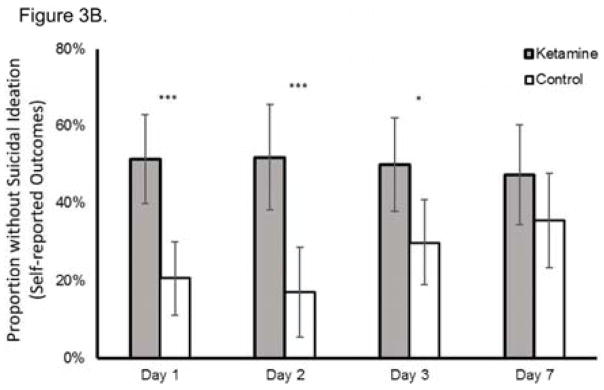
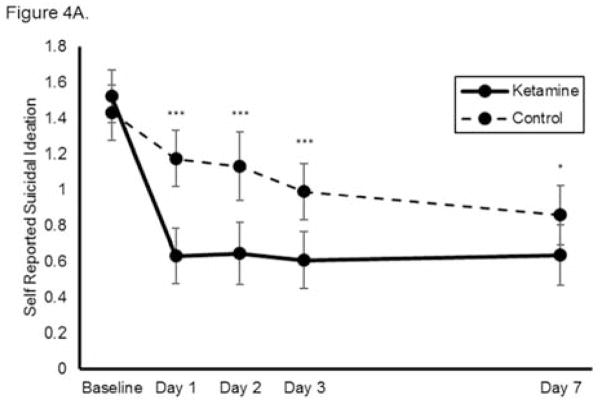
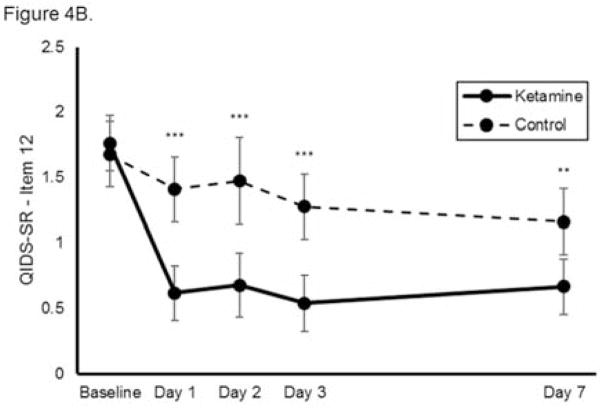
Results: Ketamine rapidly (within 1 day) reduced suicidal ideation significantly on both the clinician-administered and self-report outcome measures. Effect sizes were moderate to large (Cohen's d=0.48-0.85) at all time points after dosing. A sensitivity analysis demonstrated that compared with control treatments, ketamine had significant benefits on the individual suicide items of the MADRS, the HAM-D, and the QIDS-SR but not the BDI. Ketamine's effect on suicidal ideation remained significant after adjusting for concurrent changes in severity of depressive symptoms.
Conclusions: Ketamine rapidly reduced suicidal thoughts, within 1 day and for up to 1 week in depressed patients with suicidal ideation. Ketamine's effects on suicidal ideation were partially independent of its effects on mood, although subsequent trials in transdiagnostic samples are required to confirm that ketamine exerts a specific effect on suicidal ideation. Additional research on ketamine's long-term safety and its efficacy in reducing suicide risk is needed before clinical implementation.
Keywords: Ketamine; Mood Disorders-Bipolar; Mood Disorders-Unipolar; Rapid-Acting Antidepressants; Suicide.
Figures
Comment in
-
Antisuicidal Effects of Ketamine: A Promising First Step.Am J Psychiatry. 2018 Feb 1;175(2):97-98. doi: 10.1176/appi.ajp.2017.17111261. Am J Psychiatry. 2018. PMID: 29385830 No abstract available.
References
-
- Aleman A, Denys D. Mental health: A road map for suicide research and prevention. Nature. 2014;509(7501):421–3. - PubMed
-
- Curtin SC, Warner M, Hedegaard H. Increase in Suicide in the United States, 1999–2014. NCHS Data Brief. 2016;(241):1–8. - PubMed
-
- Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33(3):395–405. - PubMed
-
- National Action Alliance for Suicide Prevention: Research Prioritization Task Force. A prioritized research agenda for suicide prevention: An action plan to save lives. Rockville, MD: National Institute of Mental Health and the Research Prioritization Task Force; 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
