

Associated factors, diagnosis and management of Acanthamoeba keratitis in a referral Center in Southern China
- PMID: 28969610
- PMCID: PMC5625641
- DOI: 10.1186/s12886-017-0571-7
Associated factors, diagnosis and management of Acanthamoeba keratitis in a referral Center in Southern China
Abstract
Background: To analyse the associated factors, diagnosis, clinical manifestations and therapeutic effects of Acanthamoeba keratitis at a tertiary ophthalmic centre in Southern China.
Methods: A retrospective clinical study was performed in fifteen patients who were admitted to Zhongshan Ophthalmic Centre (ZOC) from January 2004 to December 2014. The patients' pathogenesis-associated factors were analysed, and preoperative diagnoses were determined using corneal scraping cultures and/or confocal microscopy followed. All diagnoses were confirmed by postoperative pathological examinations. At follow-up, best-corrected visual acuity (BCVA), the recurrence rate and graft transparency were evaluated to assess therapeutic effects.
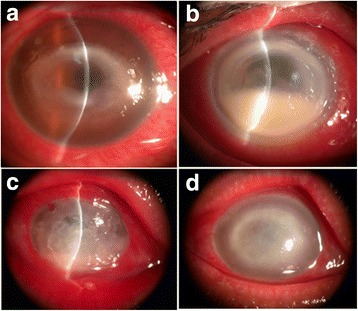
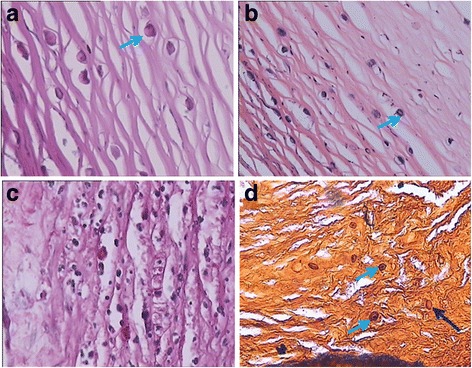
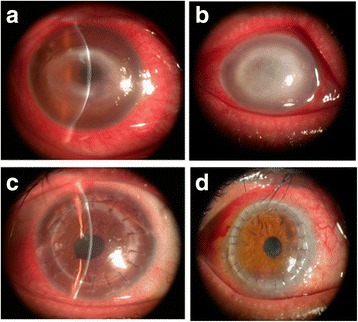
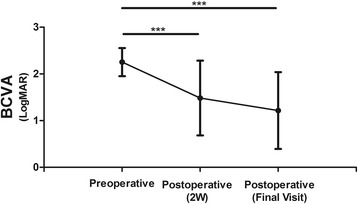
Results: The main pathogenic factors observed in the fifteen patients were a history of injury or a foreign body entering the eyes (12 cases). In all, Acanthamoeba keratitis was preoperatively diagnosed in 5 cases using corneal scraping cultures or confocal microscopy. Ocular symptoms included redness, photophobia, tearing, and blurred vision. Penetrating keratoplasty was performed in thirteen patients, and postoperative pathological examinations were performed to confirm these diagnoses. The logarithm of the minimum angle of resolution (logMAR) of visual acuity was significantly improved after keratoplasty (p < 0.01). No recurrence was observed, and approximately 90% of the corneal grafts were found to be transparent during the follow-up period.
Conclusions: Corneal trauma may be the main pathogenic factor that causes Acanthamoeba keratitis in southern China. Corneal scraping combined with confocal microscopy was helpful for achieving a correct diagnosis. Early keratoplasty combined with amoebicidal therapy is an effective treatment strategy in Acanthamoeba keratitis.
Keywords: Acanthamoeba keratitis; Associated factors; Diagnosis; Keratoplasty.
Conflict of interest statement
Ethics approval and consent to participate
Our study was performed in a manner consistent with the tenets of the Declaration of Helsinki. All medical records were anonymized, and all information was used only for research purposes. All persons enrolled provided informed consent prior to their inclusion in the study. The study was approved by the Investigational Review Board of Zhongshan Ophthalmic Centre, Sun Yat-sen University, Guangzhou, China.
Consent for publication
All authors consent to the publication of this manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Jones DB, Visvesvara GS, Robinson NM. Acanthamoeba polyphaga keratitis and Acenthamoeba uveitis associated with fatal meningoencephalitis. Trans Ophthalmol Soc UK. 1975;95:221–232. - PubMed
-
- Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009.Am J Ophthalmol. 2009 Oct;148(4):487–499.e2. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
