

Results of the 2016 International Skin Imaging Collaboration International Symposium on Biomedical Imaging challenge: Comparison of the accuracy of computer algorithms to dermatologists for the diagnosis of melanoma from dermoscopic images
- PMID: 28969863
- PMCID: PMC5768444
- DOI: 10.1016/j.jaad.2017.08.016
Results of the 2016 International Skin Imaging Collaboration International Symposium on Biomedical Imaging challenge: Comparison of the accuracy of computer algorithms to dermatologists for the diagnosis of melanoma from dermoscopic images
Abstract
Background: Computer vision may aid in melanoma detection.
Objective: We sought to compare melanoma diagnostic accuracy of computer algorithms to dermatologists using dermoscopic images.
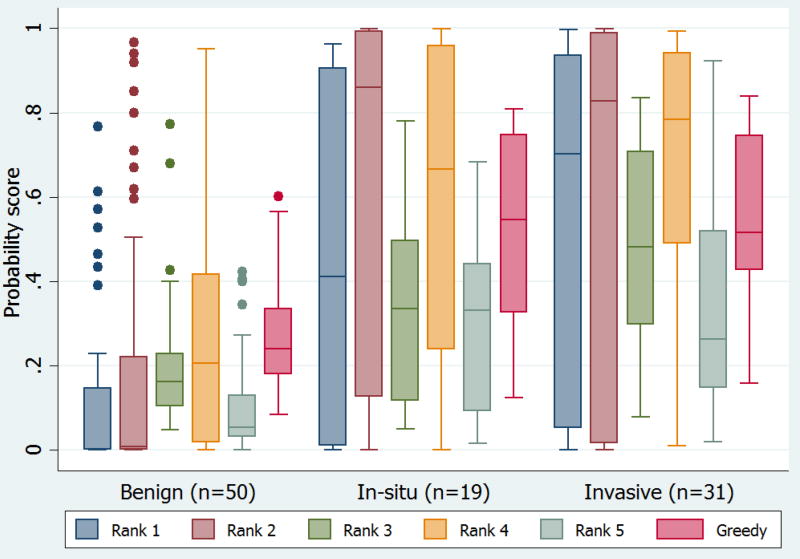
Methods: We conducted a cross-sectional study using 100 randomly selected dermoscopic images (50 melanomas, 44 nevi, and 6 lentigines) from an international computer vision melanoma challenge dataset (n = 379), along with individual algorithm results from 25 teams. We used 5 methods (nonlearned and machine learning) to combine individual automated predictions into "fusion" algorithms. In a companion study, 8 dermatologists classified the lesions in the 100 images as either benign or malignant.
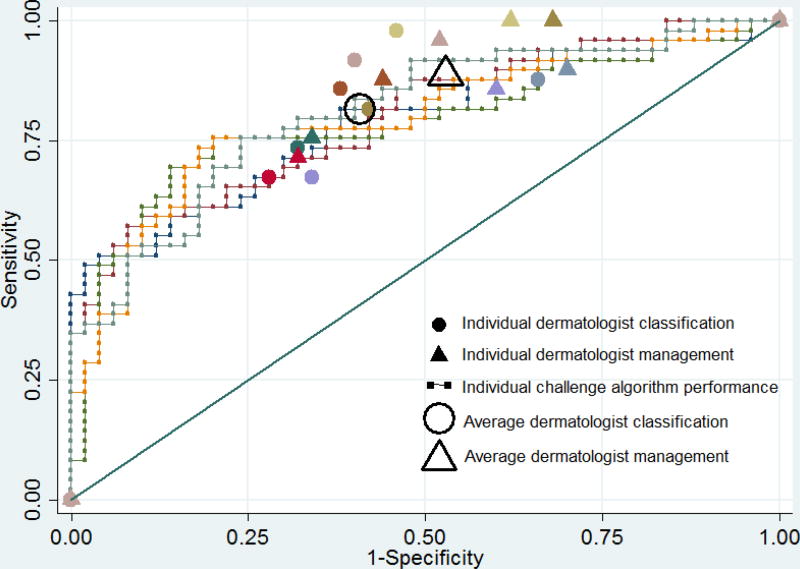
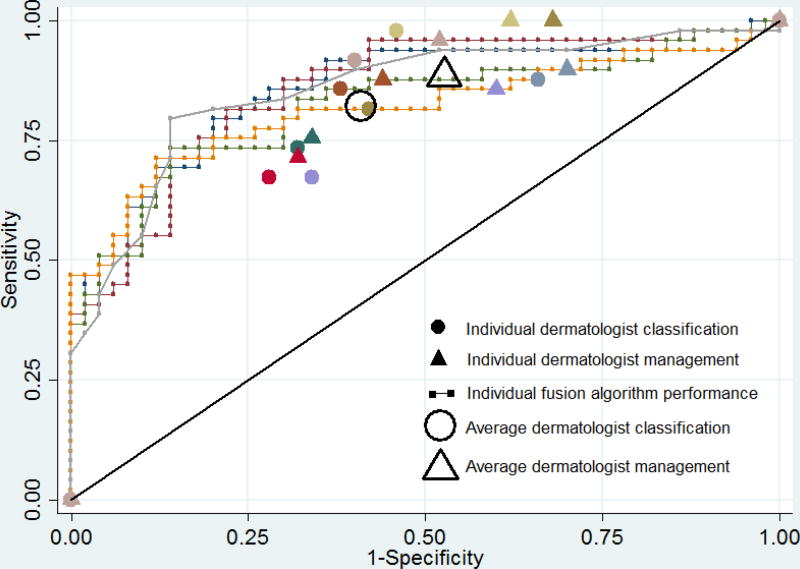
Results: The average sensitivity and specificity of dermatologists in classification was 82% and 59%. At 82% sensitivity, dermatologist specificity was similar to the top challenge algorithm (59% vs. 62%, P = .68) but lower than the best-performing fusion algorithm (59% vs. 76%, P = .02). Receiver operating characteristic area of the top fusion algorithm was greater than the mean receiver operating characteristic area of dermatologists (0.86 vs. 0.71, P = .001).
Limitations: The dataset lacked the full spectrum of skin lesions encountered in clinical practice, particularly banal lesions. Readers and algorithms were not provided clinical data (eg, age or lesion history/symptoms). Results obtained using our study design cannot be extrapolated to clinical practice.
Conclusion: Deep learning computer vision systems classified melanoma dermoscopy images with accuracy that exceeded some but not all dermatologists.
Keywords: International Skin Imaging Collaboration; International Symposium on Biomedical Imaging; computer algorithm; computer vision; dermatologist; machine learning; melanoma; reader study; skin cancer.
Copyright © 2017 American Academy of Dermatology, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Marghoob AA, Scope A. The complexity of diagnosing melanoma. J Invest Dermatol. 2009;129(1):11–13. - PubMed
-
- Monheit G, Cognetta AB, Ferris L, et al. The performance of MelaFind: a prospective multicenter study. Arch Dermatol. 2011;147(2):188–194. - PubMed
-
- Brady MS, Oliveria SA, Christos PJ, et al. Patterns of detection in patients with cutaneous melanoma. Cancer. 2000;89(2):342–347. - PubMed
-
- Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for Skin Cancer: US Preventive Services Task Force Recommendation Statement. Jama. 2016;316(4):429–435. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
