

Preoperative next-generation sequencing of pancreatic cyst fluid is highly accurate in cyst classification and detection of advanced neoplasia
- PMID: 28970292
- PMCID: PMC6241612
- DOI: 10.1136/gutjnl-2016-313586
Preoperative next-generation sequencing of pancreatic cyst fluid is highly accurate in cyst classification and detection of advanced neoplasia
Abstract
Objective: DNA-based testing of pancreatic cyst fluid (PCF) is a useful adjunct to the evaluation of pancreatic cysts (PCs). Mutations in KRAS/GNAS are highly specific for intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms (MCNs), while TP53/PIK3CA/PTEN alterations are associated with advanced neoplasia. A prospective study was performed to evaluate preoperative PCF DNA testing.
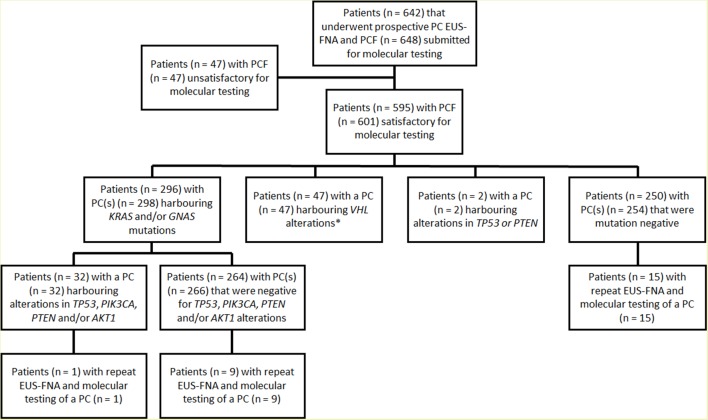
Design: Over 43-months, 626 PCF specimens from 595 patients were obtained by endoscopic ultrasound (EUS)-fine needle aspiration and assessed by targeted next-generation sequencing (NGS). Molecular results were correlated with EUS findings, ancillary studies and follow-up. A separate cohort of 159 PCF specimens was also evaluated for KRAS/GNAS mutations by Sanger sequencing.
Results: KRAS/GNAS mutations were identified in 308 (49%) PCs, while alterations in TP53/PIK3CA/PTEN were present in 35 (6%) cases. Based on 102 (17%) patients with surgical follow-up, KRAS/GNAS mutations were detected in 56 (100%) IPMNs and 3 (30%) MCNs, and associated with 89% sensitivity and 100% specificity for a mucinous PC. In comparison, KRAS/GNAS mutations by Sanger sequencing had a 65% sensitivity and 100% specificity. By NGS, the combination of KRAS/GNAS mutations and alterations in TP53/PIK3CA/PTEN had an 89% sensitivity and 100% specificity for advanced neoplasia. Ductal dilatation, a mural nodule and malignant cytopathology had lower sensitivities (42%, 32% and 32%, respectively) and specificities (74%, 94% and 98%, respectively).
Conclusions: In contrast to Sanger sequencing, preoperative NGS of PCF for KRAS/GNAS mutations is highly sensitive for IPMNs and specific for mucinous PCs. In addition, the combination of TP53/PIK3CA/PTEN alterations is a useful preoperative marker for advanced neoplasia.
Keywords: pancreatic cancer; pancreatic epidemiology; pancreatic pathology; pancreato-biliary disorders.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Towards optimal pancreatic cyst fluid management: the need for standardisation.Gut. 2019 Oct;68(10):1906. doi: 10.1136/gutjnl-2018-317156. Epub 2018 Oct 9. Gut. 2019. PMID: 30301772 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous