

Concomitant Reverse Hill-Sachs Lesion and Posterior Humeral Avulsion of the Glenohumeral Ligament: Treatment With Fresh Talus Osteochondral Allograft and Arthroscopic Posterior Humeral Avulsion of the Glenohumeral Ligament and Labrum Repair
- PMID: 28970982
- PMCID: PMC5621160
- DOI: 10.1016/j.eats.2017.03.012
Concomitant Reverse Hill-Sachs Lesion and Posterior Humeral Avulsion of the Glenohumeral Ligament: Treatment With Fresh Talus Osteochondral Allograft and Arthroscopic Posterior Humeral Avulsion of the Glenohumeral Ligament and Labrum Repair
Abstract
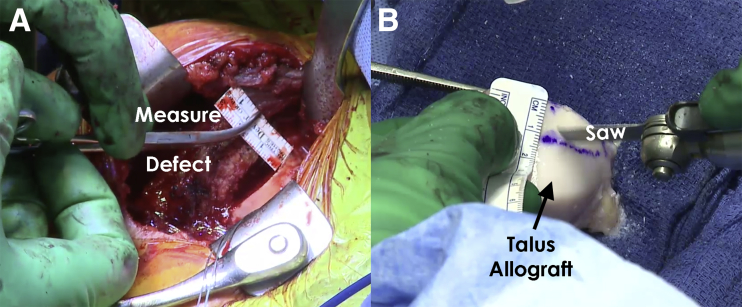
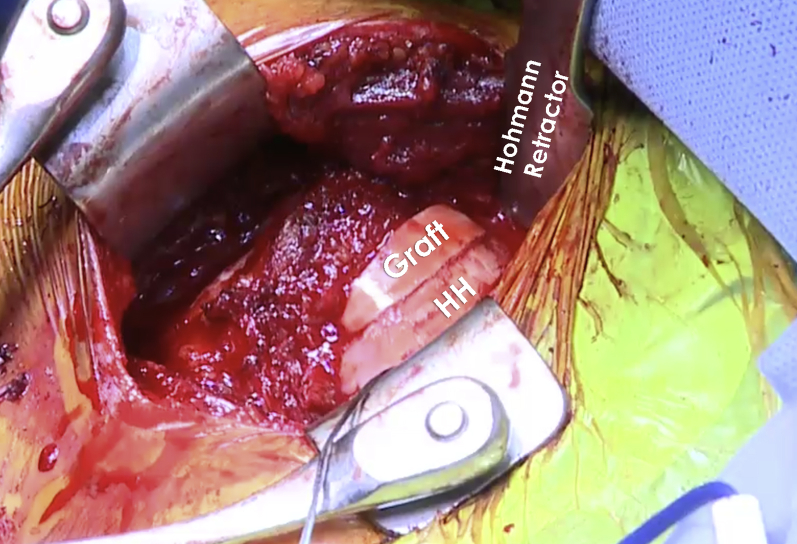
Chronic posterior glenohumeral joint instability can be a challenging clinical entity for patients and surgeons alike. In the setting of a posterior dislocation, a large anterior humeral impaction injury (reverse Hill-Sachs [HS]) may occur, leading to engagement of the humerus with the posterior glenoid bone, especially during internal rotation of the joint. A reverse HS is especially debilitating because of the significant portion of affected humeral head cartilage, and is made worse in the setting of ligamentous disruption such as a posterior humeral avulsion of the glenohumeral ligament (HAGL) lesions. Although several nonanatomic procedures to address these defects have been previously described, recent interest in anatomic reconstructions capable of restoring the cartilage surface of the humeral head has led to the use of bone grafts (autografts and allografts) to restore the articular contour of the humeral head in conjunction with anatomic repair of associated soft tissue injuries. We present our preferred technique for an anatomic repair of a posterior HAGL lesion in combination with reconstruction of an engaging reverse HS lesion using an unmatched hemitalar allograft.
Figures





Similar articles
-
Multidirectional Shoulder Instability With Circumferential Labral Tear and Bony Reverse Hill Sachs: Treatment with 270° Labral Repair and Fresh Talus Osteochondral Allograft to the Humeral Head.Arthrosc Tech. 2021 Feb 15;10(3):e781-e787. doi: 10.1016/j.eats.2020.10.068. eCollection 2021 Mar. Arthrosc Tech. 2021. PMID: 33738215 Free PMC article.
-
Anatomic Humeral Head Reconstruction With Fresh Osteochondral Talus Allograft for Recurrent Glenohumeral Instability With Reverse Hill-Sachs Lesion.Arthrosc Tech. 2017 Feb 27;6(1):e255-e261. doi: 10.1016/j.eats.2016.10.017. eCollection 2017 Feb. Arthrosc Tech. 2017. PMID: 28409110 Free PMC article.
-
The effect of a combined glenoid and Hill-Sachs defect on glenohumeral stability: a biomechanical cadaveric study using 3-dimensional modeling of 142 patients.Am J Sports Med. 2015 Jun;43(6):1422-9. doi: 10.1177/0363546515574677. Epub 2015 Mar 20. Am J Sports Med. 2015. PMID: 25794869
-
Humeral Avulsion of the Glenohumeral Ligament: Indications for Surgical Treatment and Outcomes-A Systematic Review.Orthop J Sports Med. 2017 Aug 14;5(8):2325967117723329. doi: 10.1177/2325967117723329. eCollection 2017 Aug. Orthop J Sports Med. 2017. PMID: 28840152 Free PMC article. Review.
-
Allograft reconstruction for humeral head defects in the setting of shoulder instability: a systematic review.JSES Rev Rep Tech. 2022 Aug 7;2(4):489-496. doi: 10.1016/j.xrrt.2022.07.001. eCollection 2022 Nov. JSES Rev Rep Tech. 2022. PMID: 37588454 Free PMC article. Review.
Cited by
-
Talar Allograft Preparation for Treatment of Reverse Hill-Sachs Defect in Recurrent Posterior Shoulder Instability.Arthrosc Tech. 2022 Sep 21;11(9):e1625-e1631. doi: 10.1016/j.eats.2022.05.009. eCollection 2022 Sep. Arthrosc Tech. 2022. PMID: 36185122 Free PMC article.
-
Humeral Head Reconstruction With Osteochondral Allograft: Bone Plug Optimization for Hill-Sachs Lesions Using CT-Based Computer Modeling Analysis.Orthop J Sports Med. 2023 Sep 6;11(9):23259671231193768. doi: 10.1177/23259671231193768. eCollection 2023 Sep. Orthop J Sports Med. 2023. PMID: 37693809 Free PMC article.
-
Minced Cartilage Procedure for One-Stage Arthroscopic Repair of Chondral Defects at the Glenohumeral Joint.Arthrosc Tech. 2021 Jun 20;10(7):e1677-e1684. doi: 10.1016/j.eats.2021.03.012. eCollection 2021 Jul. Arthrosc Tech. 2021. PMID: 34354912 Free PMC article.
-
Chronic locked posterior gleno-humeral dislocation: technical note on fibular grafting for restoration of humeral head sphericity.J Orthop Surg Res. 2021 Nov 18;16(1):683. doi: 10.1186/s13018-021-02835-2. J Orthop Surg Res. 2021. PMID: 34794483 Free PMC article.
-
Articular Cartilage Defects of the Glenohumeral Joint: A Systematic Review of Treatment Options and Outcomes.Cartilage. 2021 Dec;13(1_suppl):401S-413S. doi: 10.1177/1947603519870858. Epub 2019 Aug 23. Cartilage. 2021. PMID: 31441316 Free PMC article.
References
-
- Owens B.D., Campbell S.E., Cameron K.L. Risk factors for posterior shoulder instability in young athletes. Am J Sports Med. 2013;41:2645–2649. - PubMed
-
- Owens B.D., Duffey M.L., Nelson B.J., DeBerardino T.M., Taylor D.C., Mountcastle S.B. The incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007;35:1168–1173. - PubMed
-
- Saupe N., White L.M., Bleakney R. Acute traumatic posterior shoulder dislocation: MR findings. Radiology. 2008;248:185–193. - PubMed
-
- Moroder P., Tauber M., Scheibel M. Defect characteristics of reverse Hill-Sachs lesions. Am J Sports Med. 2016;44:708–714. - PubMed
-
- Bui-Mansfield L.T., Banks K.P., Taylor D.C. Humeral avulsion of the glenohumeral ligaments: The HAGL lesion. Am J Sports Med. 2007;35:1960–1966. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
