

doi: 10.1016/j.eats.2017.03.009.
eCollection 2017 Aug.
Arthroscopic Revision of Medial Rotator Cuff Failure Augmented With a Bioabsorbable Patch
Affiliations
- PMID: 28970994
- PMCID: PMC5621132
- DOI: 10.1016/j.eats.2017.03.009
Item in Clipboard
Arthroscopic Revision of Medial Rotator Cuff Failure Augmented With a Bioabsorbable Patch
Arthrosc Tech.
.
Abstract
When revising failed double-row and suture-bridge rotator cuff repairs medial failures represent a potential feature. In the presence of a compromised healing environment, patch augmentation becomes a logical adjunct from a mechanical and biological point of view. A reproducible step-by-step revision technique is described that reinforces the weak central cuff area with an absorbable synthetic scaffold.
Figures

Patient in the beach-chair position, right shoulder: set-up and main working portals; trocar introduced into the glenohumeral joint from the posterior standard portal.

Right shoulder, lateral viewing portal. (A) Arthroscopic view of the debrided footprint. (B) Anchor with 3 sutures has been inserted at the articular margin. (C) Suture-bridge repair has closed the defect. (FP, footprint; ISP, infraspinatus; SB, suture-bridge; SSP, supraspinatus; TA, triple-loaded anchor.)

(A) Right shoulder, lateral view. Diagram of suture passage after footprint preparation and anchor insertion. Side-to-side (blue) PDS sutures at the apex of the tear passed with a straight Spectrum needle. Anchor sutures are passed with Clever hooks; the posterior mattress suture (dark green) includes a deep layer of ISP. Light green and blue anchor sutures work as “margin-convergence to bone.” (B) Right shoulder, lateral view. Diagram after knot tying and lateral fixation with 2 PushLock anchors. Two suture limbs are left long for lateral fixation of the patch. Optional inclusion of suture strands from SSC refixation is sketched (not shown in Video 1). Figure courtesy of Sarah Bahler (www.sarahbaehler.ch ). (ISP, infraspinatus; SSC, subscapularis; SSP, supraspinatus.)
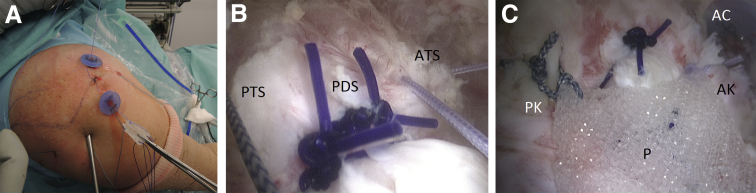
Right shoulder. (A) Picture showing pulling-in of the patch through the lateral Passport cannula; watch PDS shuttle sutures in the lateral corners. (B) Arthroscopic view from the posterolateral portal; patch is pulled into place with long Orthocord traction sutures passing at the musculotendinous junction. (C) Arthroscopic view from the lateral portal; sutures have been tied through the anterior cannula to complete medial fixation. (AC, anterior cannula; AK, anterior knot; ATS, anterior traction stitch; P, patch; PDS, margin-convergence stitches; PK, posterior knot; PTS, posterior traction stitch.)

Right shoulder, lateral viewing portal. (A) Lateral fixation with leftover suture limbs from the posterior PushLock anchor. (B) Lateral fixation completed; some tension was applied. (C) Sideward fixation with PDS stitches. (APL, anterior PushLock; P, patch; PDS, sideward stitches; PPL, posterior PushLock; SB, suture-bridge visible under patch; SL, suture limbs.)

(A) Right shoulder, lateral view. Diagram of patch transportation into subacromial space. (B) Right shoulder, lateral view. Diagram of the final aspect of the patch secured over the weak cuff area; 6 fixation points to underlying tissue. Figure courtesy of Sarah Bahler (www.sarahbaehler.ch ). (ISP, infraspinatus; SSC, subscapularis; SSP, supraspinatus.)

Right shoulder, posterolateral viewing portal. Arthroscopic image of reoperation at 6 months showing successful integration of scaffold in cuff tissue. (NC, native cuff; P, patch.)
References
-
- Mall N.A., Tanaka M.J., Choi L.S., Paletta G.A., Jr. Factors affecting rotator cuff healing. J Bone Joint Surg Am. 2014;96:778–788. - PubMed
-
- Buess E. Failures following arthroscopic rotator cuff repair. Recurrent tears, incomplete healing or central cuff failure. Arthroskopie. 2012;25:111–117. [in German]
-
- Trantalis J.N., Boorman R.S., Pletsch K., Lo I.K. Medial rotator cuff failure after arthroscopic double-row rotator cuff repair. Arthroscopy. 2008;24:727–731. - PubMed
-
- Cho N.S., Yi J.W., Lee B.G., Rhee Y.G. Retear patterns after arthroscopic rotator cuff repair: Single-row versus suture bridge technique. Am J Sports Med. 2010;38:664–671. - PubMed
-
- Ricchetti E.T., Aurora A., Iannotti J.P., Derwin K.A. Scaffold devices for rotator cuff repair. J Shoulder Elbow Surg. 2012;21:251–265. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
