

Wave intensity analysis and its application to the coronary circulation
- PMID: 28971104
- PMCID: PMC5621714
- DOI: 10.21542/gcsp.2017.5
Wave intensity analysis and its application to the coronary circulation
Abstract
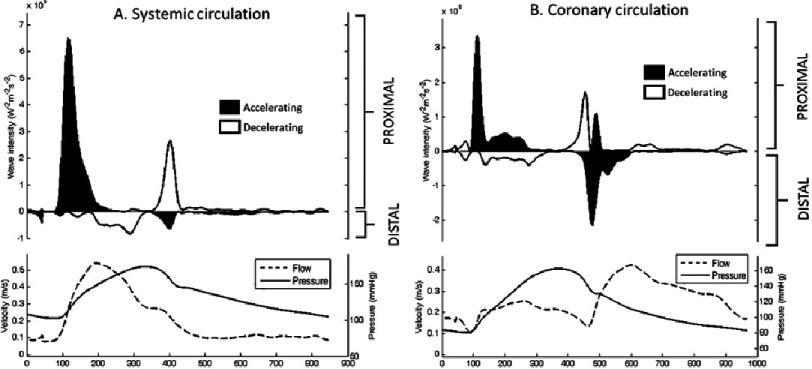
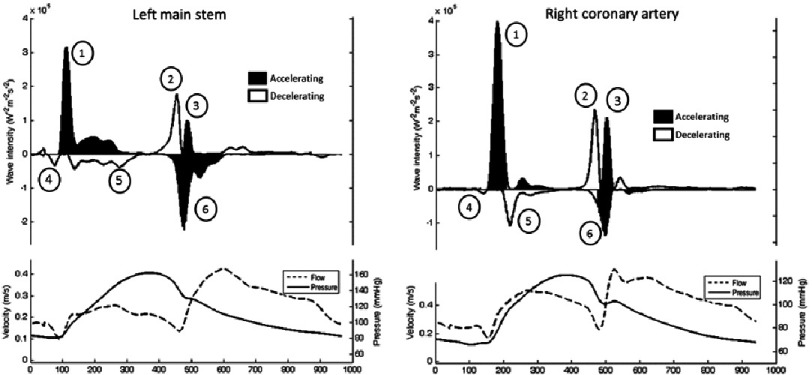
Wave intensity analysis (WIA) is a technique developed from the field of gas dynamics that is now being applied to assess cardiovascular physiology. It allows quantification of the forces acting to alter flow and pressure within a fluid system, and as such it is highly insightful in ascribing cause to dynamic blood pressure or velocity changes. When co-incident waves arrive at the same spatial location they exert either counteracting or summative effects on flow and pressure. WIA however allows waves of different origins to be measured uninfluenced by other simultaneously arriving waves. It therefore has found particular applicability within the coronary circulation where both proximal (aortic) and distal (myocardial) ends of the coronary artery can markedly influence blood flow. Using these concepts, a repeating pattern of 6 waves has been consistently identified within the coronary arteries, 3 originating proximally and 3 distally. Each has been associated with a particular part of the cardiac cycle. The most clinically relevant wave to date is the backward decompression wave, which causes the marked increase in coronary flow velocity observed at the start of the diastole. It has been proposed that this wave is generated by the elastic re-expansion of the intra-myocardial blood vessels that are compressed during systolic contraction. Particularly by quantifying this wave, WIA has been used to provide mechanistic and prognostic insight into a number of conditions including aortic stenosis, left ventricular hypertrophy, coronary artery disease and heart failure. It has proven itself to be highly sensitive and as such a number of novel research directions are encouraged where further insights would be beneficial.
Keywords: Wave intensity analysis; coronary vessels; diagnostic techniques; microcirculation; physiology.
Figures
Similar articles
-
Major influence of a 'smoke and mirrors' effect caused by wave reflection on early diastolic coronary arterial wave intensity.J Physiol. 2018 Mar 15;596(6):993-1017. doi: 10.1113/JP274710. Epub 2018 Feb 13. J Physiol. 2018. PMID: 29318640 Free PMC article.
-
Estimation of coronary wave intensity analysis using noninvasive techniques and its application to exercise physiology.Am J Physiol Heart Circ Physiol. 2016 Mar 1;310(5):H619-27. doi: 10.1152/ajpheart.00575.2015. Epub 2015 Dec 18. Am J Physiol Heart Circ Physiol. 2016. PMID: 26683900 Free PMC article.
-
Transcatheter Replacement of Stenotic Aortic Valve Normalizes Cardiac-Coronary Interaction by Restoration of Systolic Coronary Flow Dynamics as Assessed by Wave Intensity Analysis.Circ Cardiovasc Interv. 2016 Apr;9(4):e002356. doi: 10.1161/CIRCINTERVENTIONS.114.002356. Circ Cardiovasc Interv. 2016. PMID: 27001805
-
Haemodynamic basis for the development of left ventricular failure in systolic hypertension and for its logical therapy.J Hypertens. 1995 Sep;13(9):943-52. doi: 10.1097/00004872-199509000-00002. J Hypertens. 1995. PMID: 8586828 Review.
-
Arterial elastance and wave reflection augmentation of systolic blood pressure: deleterious effects and implications for therapy.J Cardiovasc Pharmacol Ther. 2001 Jan;6(1):5-21. doi: 10.1177/107424840100600102. J Cardiovasc Pharmacol Ther. 2001. PMID: 11452332 Review.
Cited by
-
Altered cardiac-coronary coupling relates to abnormal fractional flow reserve without flow limitation after percutaneous coronary interventions.Physiol Rep. 2025 Jul;13(13):e70440. doi: 10.14814/phy2.70440. Physiol Rep. 2025. PMID: 40588683 Free PMC article.
-
A computational study of aortic reconstruction in single ventricle patients.Biomech Model Mechanobiol. 2023 Feb;22(1):357-377. doi: 10.1007/s10237-022-01650-w. Epub 2022 Nov 5. Biomech Model Mechanobiol. 2023. PMID: 36335184 Free PMC article.
-
Feasibility of Wave Intensity Analysis from 4D Cardiovascular Magnetic Resonance Imaging Data.Bioengineering (Basel). 2023 May 31;10(6):662. doi: 10.3390/bioengineering10060662. Bioengineering (Basel). 2023. PMID: 37370593 Free PMC article.
-
Opposing forces and a river into a lake: Relevance to coronary hemodynamics in Kawasaki disease.Glob Cardiol Sci Pract. 2017 Oct 31;2017(3):e201719. doi: 10.21542/gcsp.2017.19. Glob Cardiol Sci Pract. 2017. PMID: 29564340 Free PMC article. No abstract available.
-
Energetics of flow restoration after premature ventricular contractions depends on microvascular vasodilation capacity: Insights from wave intensity analysis.Eur Heart J Open. 2025 Apr 15;5(3):oeaf041. doi: 10.1093/ehjopen/oeaf041. eCollection 2025 May. Eur Heart J Open. 2025. PMID: 40342910 Free PMC article. No abstract available.
References
-
- Davies JE, Whinnett ZI, Francis DP, Manisty CH, Aguado-Sierra J, Willson K, Foale RA, Malik IS, Hughes AD, Parker KH, Mayet J. Evidence of a dominant backward-propagating “suction” wave responsible for diastolic coronary filling in humans, attenuated in left ventricular hypertrophy. Circulation. 2006;113(14):1768–1778. - PubMed
-
- Davies JE, Sen S, Broyd C, Hadjiloizou N, Baksi J, Francis DP, Foale RA, Parker KH, Hughes AD, Chukwuemeka A, Casula R, Malik IS, Mikhail GW, Mayet J. Arterial pulse wave dynamics after percutaneous aortic valve replacement: Fall in coronary diastolic suction with increasing heart rate as a basis for angina symptoms in aortic stenosis. Circulation. 2011;124(14):1565–1572. - PubMed
-
- Silva K De, Guilcher A, Lockie T, Marber M, Redwood S, Plein S, Perera D. Coronary wave intensity: A novel invasive tool for predicting myocardial viability following acute coronary syndromes. J Am Coll Cardiol. 2012;59(13s1):E421–E421.
-
- Lockie TP, Rolandi MC, Guilcher A, Perera D, De Silva K, Williams R, Asrress KN, Patel K, Plein S, Chowienczyk P, Siebes M, Redwood SR, Marber MS. Synergistic adaptations to exercise in the systemic and coronary circulations that underlie the warm-up angina phenomenon. Circulation. 2012;126(22):2565–2574. - PubMed
-
- Kyriacou A, Whinnett ZI, Sen S, Pabari PA, Wright I, Cornelussen R, Lefroy D, Davies DW, Peters NS, Kanagaratnam P, Mayet J, Hughes AD, Francis DP, Davies JE. Improvement in coronary blood flow velocity with acute biventricular pacing is predominantly due to an increase in a diastolic backward-travelling decompression (suction) wave. Circulation. 2012;126(11):1334–1344. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources