

Comparison of up-front treatments for newly diagnosed immune thrombocytopenia -a systematic review and network meta-analysis
- PMID: 28971908
- PMCID: PMC5777203
- DOI: 10.3324/haematol.2017.174615
Comparison of up-front treatments for newly diagnosed immune thrombocytopenia -a systematic review and network meta-analysis
Abstract
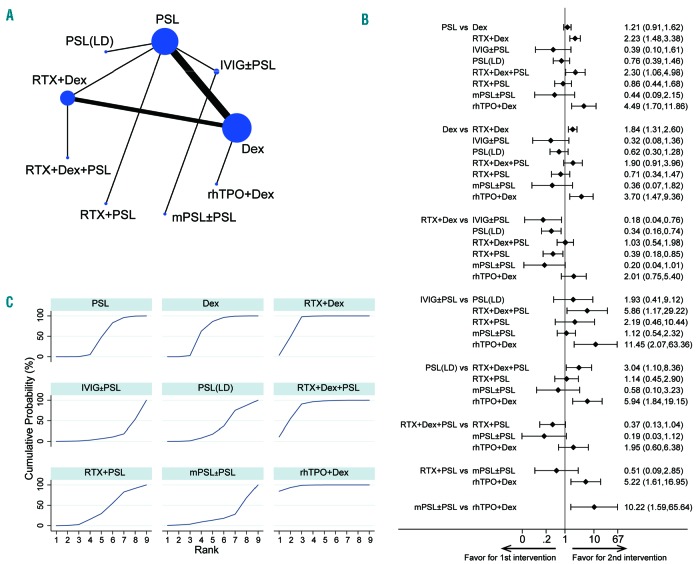
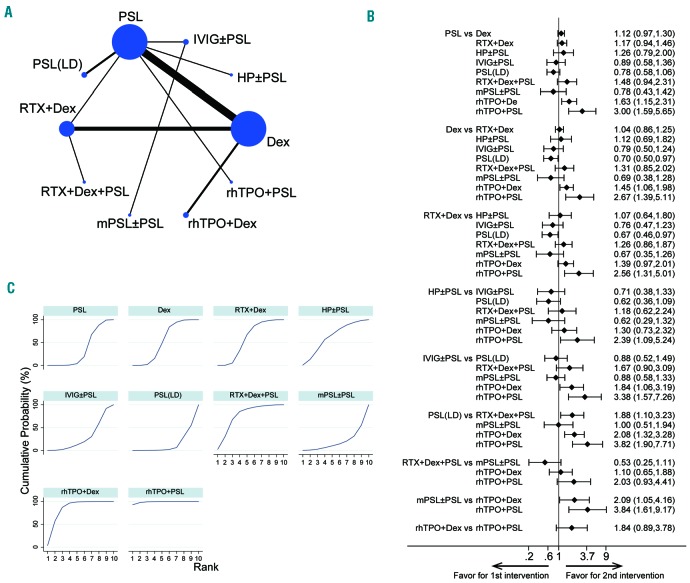
Corticosteroids such as prednisolone and dexamethasone have been established as up-front therapy for the treatment of newly diagnosed immune thrombocytopenia. Recent studies have indicated that other treatments such as rituximab or thrombopoietin receptor agonist can also be effective choices. We performed a systematic review and network meta-analysis to establish a clinically meaningful hierarchy of efficacy and safety of treatments for newly diagnosed primary immune thrombocytopenia in adults. Randomized controlled trials evaluating medical treatments for newly diagnosed immune thrombocytopenia were included. Reviewers independently extracted data and assessed the risk of bias. The main outcome was the sustained response (platelet count >30×109/L for 3-6 months after completion of treatments), while overall response (platelet count >30×109/L for 2-4 weeks after initiation of the up-front treatment) and therapy-related adverse events were the secondary endpoints. A total of 21 randomized controlled trials (1898 patients) were included in this study. Our main findings were a significantly better sustained response in the recombinant human thrombopoietin+dexamethasone and rituximab+dexamethasone arms compared to those of conventional therapies (prednisolone and dexamethasone monotherapy). Moreover, recombinant human thrombopoietin+dexamethasone and +prednisolone improved early overall response compared to prednisolone, dexamethasone, and rituximab-containing regimens. Therapy-related adverse events showed similar profiles and were tolerable in all treatment arms. Regimens containing recombinant human thrombopoietin agonist may be beneficial up-front therapies in addition to the conventional corticosteroid monotherapies. Future head-to-head trials including these regimens and rituximab-containing treatments are necessary in order to overcome the limitations of the small number in our study and determine the most suitable initial therapies for newly diagnosed immune thrombocytopenia.
Copyright© 2018 Ferrata Storti Foundation.
Figures
Comment in
-
Comment to the article by Arai Y, Jo T, Matsui H, Kondo T and Takaori-Kondo A: "Comparison of up-front treatments for newly diagnosed immune thrombocytopenia - a systematic review and network meta-analysis". Haematologica 2018;103(1):163-171. Need to direct immune thrombocytopenia therapy towards shared goals.Haematologica. 2018 Jun;103(6):e268. doi: 10.3324/haematol.2018.189183. Haematologica. 2018. PMID: 29866889 Free PMC article. No abstract available.
-
Response to the Comment by Cirasino L and Semeraro S: "Need to direct immune thrombocytopenia therapy towards shared goals" Direct and indirect comparisons to determine the first choice for newly diagnosed primary immune thrombocytopenia in adults.Haematologica. 2018 Jun;103(6):e269. doi: 10.3324/haematol.2018.192385. Haematologica. 2018. PMID: 29866890 Free PMC article. No abstract available.
References
-
- Psaila B, Bussel JB. Immune thrombocytopenic purpura. Hematol Oncol Clin North Am. 2007;21(4):743–759. - PubMed
-
- Stasi R, Evangelista ML, Stipa E, Buccisano F, Venditti A, Amadori S. Idiopathic thrombocytopenic purpura: current concepts in pathophysiology and management. Thromb Haemost. 2008;99(1):4–13. - PubMed
-
- Cohen YC, Djulbegovic B, Shamai-Lubovitz O, Mozes B. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Arch Intern Med. 2000;160(11): 1630–1638. - PubMed
-
- Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168–186. - PubMed
-
- Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood. 2011;117(16): 4190–4207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
