

Direct Comparison of Cardiac Myosin-Binding Protein C With Cardiac Troponins for the Early Diagnosis of Acute Myocardial Infarction
- PMID: 28972002
- PMCID: PMC5642333
- DOI: 10.1161/CIRCULATIONAHA.117.028084
Direct Comparison of Cardiac Myosin-Binding Protein C With Cardiac Troponins for the Early Diagnosis of Acute Myocardial Infarction
Erratum in
-
Correction to: Direct Comparison of Cardiac Myosin-Binding Protein C With Cardiac Troponins for the Early Diagnosis of Acute Myocardial Infarction.Circulation. 2017 Dec 19;136(25):e469. doi: 10.1161/CIR.0000000000000552. Circulation. 2017. PMID: 29255134 Free PMC article. No abstract available.
Abstract
Background: Cardiac myosin-binding protein C (cMyC) is a cardiac-restricted protein that is more abundant than cardiac troponins (cTn) and is released more rapidly after acute myocardial infarction (AMI). We evaluated cMyC as an adjunct or alternative to cTn in the early diagnosis of AMI.
Methods: Unselected patients (N=1954) presenting to the emergency department with symptoms suggestive of AMI, concentrations of cMyC, and high-sensitivity (hs) and standard-sensitivity cTn were measured at presentation. The final diagnosis of AMI was independently adjudicated using all available clinical and biochemical information without knowledge of cMyC. The prognostic end point was long-term mortality.
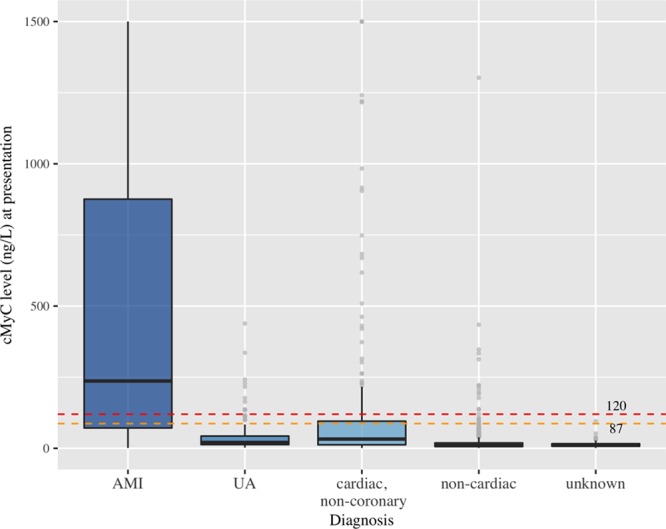
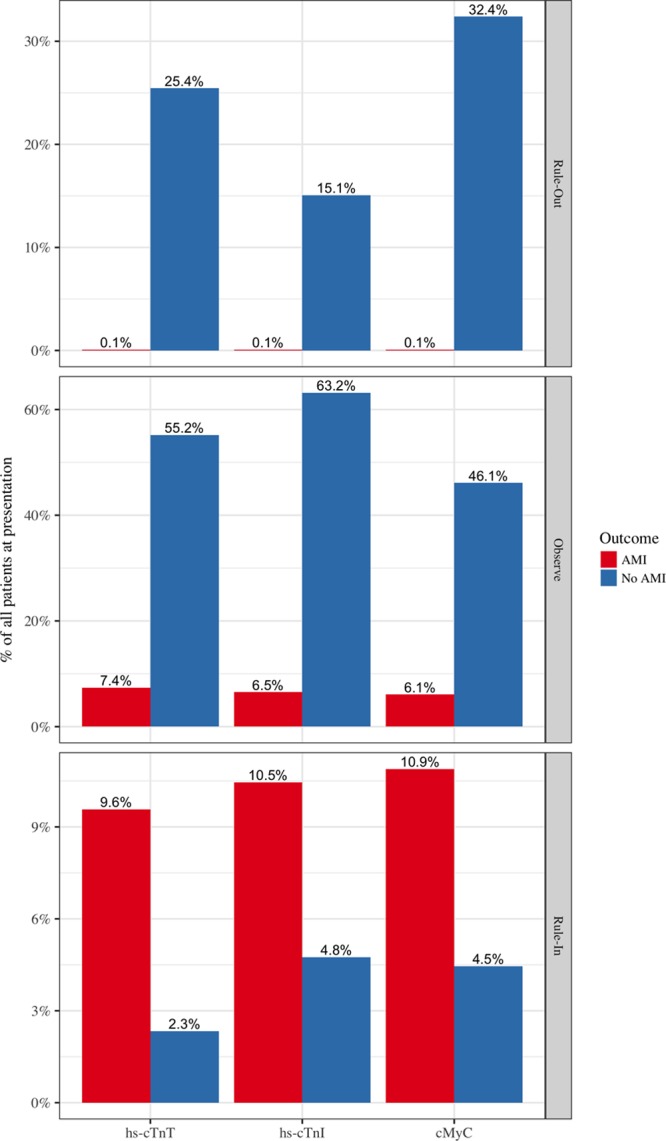
Results: Final diagnosis was AMI in 340 patients (17%). Concentrations of cMyC at presentation were significantly higher in those with versus without AMI (median, 237 ng/L versus 13 ng/L, P<0.001). Discriminatory power for AMI, as quantified by the area under the receiver-operating characteristic curve (AUC), was comparable for cMyC (AUC, 0.924), hs-cTnT (AUC, 0.927), and hs-cTnI (AUC, 0.922) and superior to cTnI measured by a contemporary sensitivity assay (AUC, 0.909). The combination of cMyC with hs-cTnT or standard-sensitivity cTnI (but not hs-cTnI) led to an increase in AUC to 0.931 (P<0.0001) and 0.926 (P=0.003), respectively. Use of cMyC more accurately classified patients with a single blood test into rule-out or rule-in categories: Net Reclassification Improvement +0.149 versus hs-cTnT, +0.235 versus hs-cTnI (P<0.001). In early presenters (chest pain <3 h), the improvement in rule-in/rule-out classification with cMyC was larger compared with hs-cTnT (Net Reclassification Improvement +0.256) and hs-cTnI (Net Reclassification Improvement +0.308; both P<0.001). Comparing the C statistics, cMyC was superior to hs-cTnI and standard sensitivity cTnI (P<0.05 for both) and similar to hs-cTnT at predicting death at 3 years.
Conclusions: cMyC at presentation provides discriminatory power comparable to hs-cTnT and hs-cTnI in the diagnosis of AMI and may perform favorably in patients presenting early after symptom onset.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00470587.
Keywords: cMyC; cardiac myosin-binding protein C; myocardial infarction, APACE; troponin I; troponin T.
© 2017 The Authors.
Figures


Comment in
-
Response by Kaier et al to Letter Regarding Article, "Direct Comparison of Cardiac Myosin-Binding Protein C With Cardiac Troponins for the Early Diagnosis of Acute Myocardial Infarction".Circulation. 2018 Jul 31;138(5):544-545. doi: 10.1161/CIRCULATIONAHA.118.035880. Circulation. 2018. PMID: 30571528 No abstract available.
-
Letter by Jiang et al Regarding Article, "Direct Comparison of Cardiac Myosin-Binding Protein C With Cardiac Troponins for the Early Diagnosis of Acute Myocardial Infarction".Circulation. 2018 Jul 31;138(5):543. doi: 10.1161/CIRCULATIONAHA.117.032597. Circulation. 2018. PMID: 30571529 No abstract available.
References
-
- U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2012 Emergency Department Summary Tables [published online ahead of print May 3, 2017]. CDC.gov. http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2012_ed_web_tables.pdf.
-
- Katus HA, Remppis A, Neumann FJ, Scheffold T, Diederich KW, Vinar G, Noe A, Matern G, Kuebler W. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation. 1991;83:902–912. - PubMed
-
- Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, Biedert S, Schaub N, Buerge C, Potocki M, Noveanu M, Breidthardt T, Twerenbold R, Winkler K, Bingisser R, Mueller C. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361:858–867. doi: 10.1056/NEJMoa0900428. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Jr, Ganiats TG, Holmes DR, Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Smalling RW, Zieman SJ. 2014 ACC/AHA guideline for the management of patients with non–ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:e344–e426. doi: 10.1161/CIR.0000000000000134. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
