

Hypermutated Circulating Tumor DNA: Correlation with Response to Checkpoint Inhibitor-Based Immunotherapy
- PMID: 28972084
- PMCID: PMC5678984
- DOI: 10.1158/1078-0432.CCR-17-1439
Hypermutated Circulating Tumor DNA: Correlation with Response to Checkpoint Inhibitor-Based Immunotherapy
Abstract
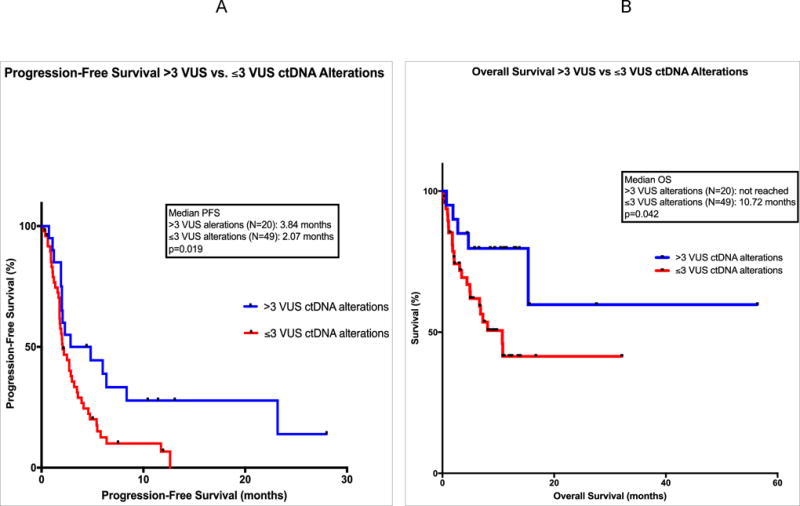
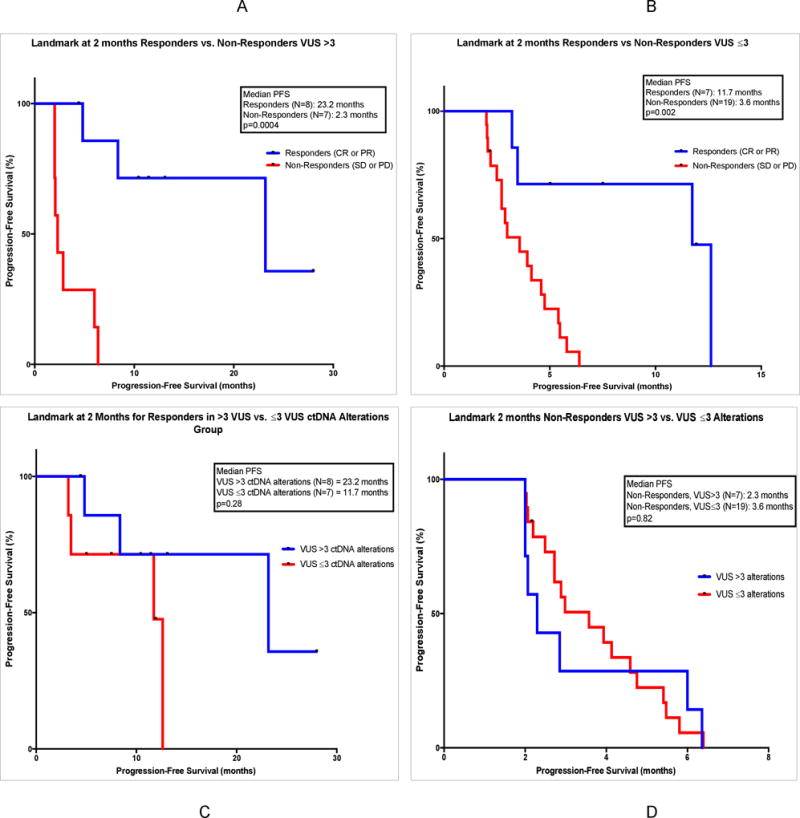
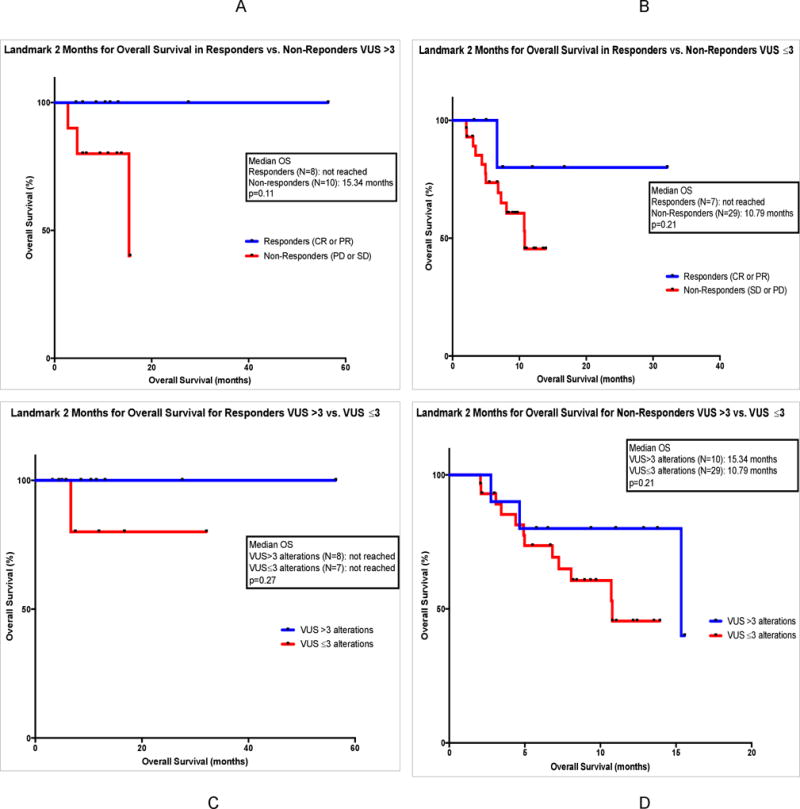
Purpose: Tumor mutational burden detected by tissue next-generation sequencing (NGS) correlates with checkpoint inhibitor response. However, tissue biopsy may be costly and invasive. We sought to investigate the association between hypermutated blood-derived circulating tumor DNA (ctDNA) and checkpoint inhibitor response.Experimental Design: We assessed 69 patients with diverse malignancies who received checkpoint inhibitor-based immunotherapy and blood-derived ctDNA NGS testing (54-70 genes). Rates of stable disease (SD) ≥6 months, partial and complete response (PR, CR), progression-free survival (PFS), and overall survival (OS) were assessed based on total and VUS alterations.Results: Statistically significant improvement in PFS was associated with high versus low alteration number in variants of unknown significance (VUS, >3 alterations versus VUS ≤3 alterations), SD ≥6 months/PR/CR 45% versus 15%, respectively; P = 0.014. Similar results were seen with high versus low total alteration number (characterized plus VUS, ≥6 vs. <6). Statistically significant OS improvement was also associated with high VUS alteration status. Two-month landmark analysis showed that responders versus nonresponders with VUS >3 had a median PFS of 23 versus 2.3 months (P = 0.0004).Conclusions: Given the association of alteration number on liquid biopsy and checkpoint inhibitor-based immunotherapy outcomes, further investigation of hypermutated ctDNA as a predictive biomarker is warranted. Clin Cancer Res; 23(19); 5729-36. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
References
-
- Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. N Engl J Med. 2015;372:2018–28. - PubMed
-
- Blumenthal GM, Pazdur R. Approvals in 2016: the march of the checkpoint inhibitors. Nat Rev Clin Oncol. 2017;14:131–2. - PubMed
-
- Goodman A, Patel SP, Kurzrock R. PD-1-PD-L1 immune-checkpoint blockade in B-cell lymphomas. Nat Rev Clin Oncol. 2017;14:203–20. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
