

A phase 3 randomized placebo-controlled trial of tadalafil for Duchenne muscular dystrophy
- PMID: 28972192
- PMCID: PMC5664308
- DOI: 10.1212/WNL.0000000000004570
A phase 3 randomized placebo-controlled trial of tadalafil for Duchenne muscular dystrophy
Abstract
Objective: To conduct a randomized trial to test the primary hypothesis that once-daily tadalafil, administered orally for 48 weeks, lessens the decline in ambulatory ability in boys with Duchenne muscular dystrophy (DMD).
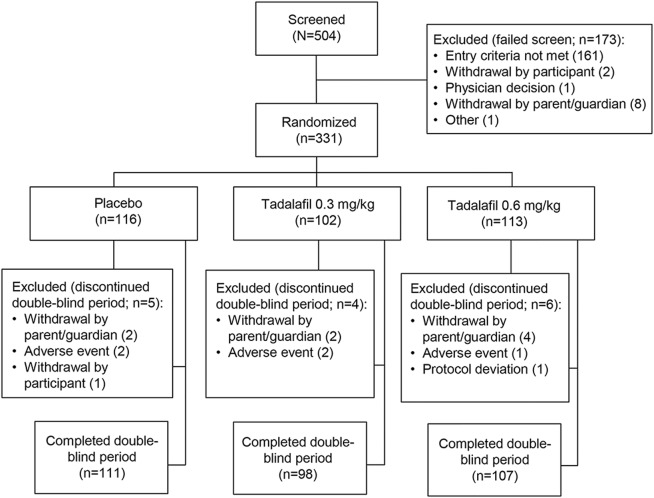
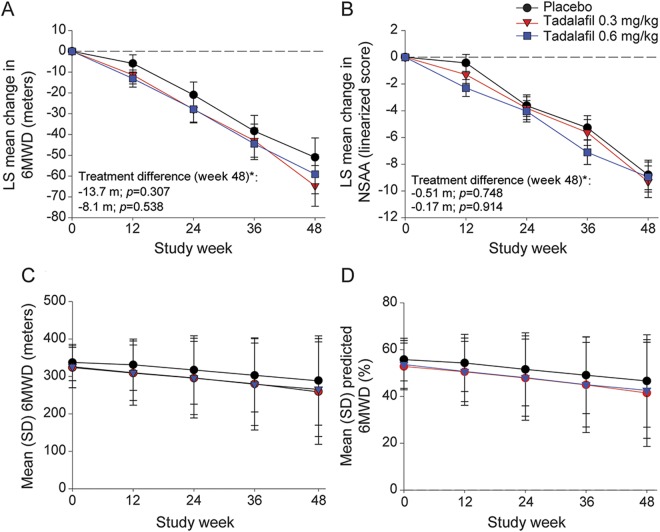
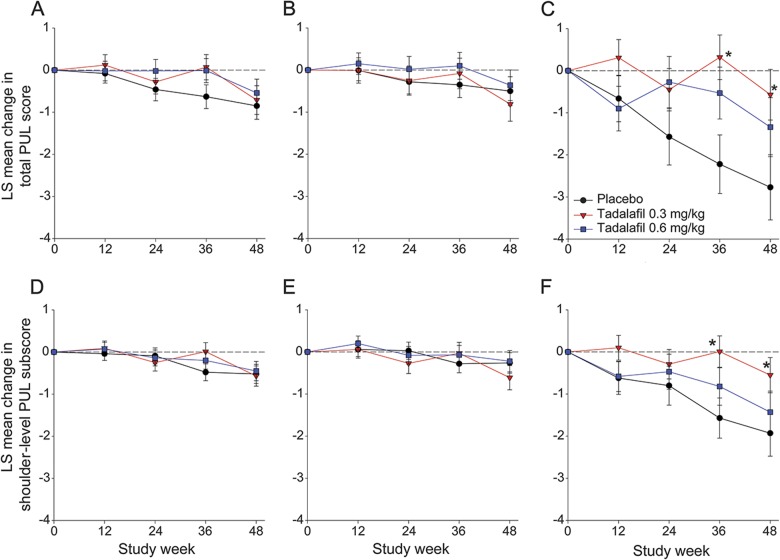
Methods: Three hundred thirty-one participants with DMD 7 to 14 years of age taking glucocorticoids were randomized to tadalafil 0.3 mg·kg-1·d-1, tadalafil 0.6 mg·kg-1·d-1, or placebo. The primary efficacy measure was 6-minute walk distance (6MWD) after 48 weeks. Secondary efficacy measures included North Star Ambulatory Assessment and timed function tests. Performance of Upper Limb (PUL) was a prespecified exploratory outcome.
Results: Tadalafil had no effect on the primary outcome: 48-week declines in 6MWD were 51.0 ± 9.3 m with placebo, 64.7 ± 9.8 m with low-dose tadalafil (p = 0.307 vs placebo), and 59.1 ± 9.4 m with high-dose tadalafil (p = 0.538 vs placebo). Tadalafil also had no effect on secondary outcomes. In boys >10 years of age, total PUL score and shoulder subscore declined less with low-dose tadalafil than placebo. Adverse events were consistent with the known safety profile of tadalafil and the DMD disease state.
Conclusions: Tadalafil did not lessen the decline in ambulatory ability in boys with DMD. Further studies should be considered to confirm the hypothesis-generating upper limb data and to determine whether ambulatory decline can be slowed by initiation of tadalafil before 7 years of age.
Clinicaltrialsgov identifier: NCT01865084.
Classification of evidence: This study provides Class I evidence that tadalafil does not slow ambulatory decline in 7- to 14-year-old boys with Duchenne muscular dystrophy.
Copyright © 2017 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Mah JK, Korngut L, Dykeman J, Day L, Pringsheim T, Jette N. A systematic review and meta-analysis on the epidemiology of Duchenne and Becker muscular dystrophy. Neuromuscul Disord 2014;24:482–491. - PubMed
-
- Ervasti JM, Ohlendieck K, Kahl SD, Gaver MG, Campbell KP. Deficiency of a glycoprotein component of the dystrophin complex in dystrophic muscle. Nature 1990;345:315–319. - PubMed
-
- Hoffman EP, Brown RH Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell 1987;51:919–928. - PubMed
-
- Brenman JE, Chao DS, Xia H, Aldape K, Bredt DS. Nitric oxide synthase complexed with dystrophin and absent from skeletal muscle sarcolemma in Duchenne muscular dystrophy. Cell 1995;82:743–752. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials