

The Ohio Contrast Cards: Visual Performance in a Pediatric Low-vision Site
- PMID: 28972542
- PMCID: PMC5626115
- DOI: 10.1097/OPX.0000000000001119
The Ohio Contrast Cards: Visual Performance in a Pediatric Low-vision Site
Abstract
Significance: This report describes the first clinical use of the Ohio Contrast Cards, a new test that measures the maximum spatial contrast sensitivity of low-vision patients who cannot recognize and identify optotypes and for whom the spatial frequency of maximum contrast sensitivity is unknown.
Purpose: To compare measurements of the Ohio Contrast Cards to measurements of three other vision tests and a vision-related quality-of-life questionnaire obtained on partially sighted students at Ohio State School for the Blind.
Methods: The Ohio Contrast Cards show printed square-wave gratings at very low spatial frequency (0.15 cycle/degree). The patient looks to the left/right side of the card containing the grating. Twenty-five students (13 to 20 years old) provided four measures of visual performance: two grating card tests (the Ohio Contrast Cards and the Teller Acuity Cards) and two letter charts (the Pelli-Robson contrast chart and the Bailey-Lovie acuity chart). Spatial contrast sensitivity functions were modeled using constraints from the grating data. The Impact of Vision Impairment on Children questionnaire measured vision-related quality of life.
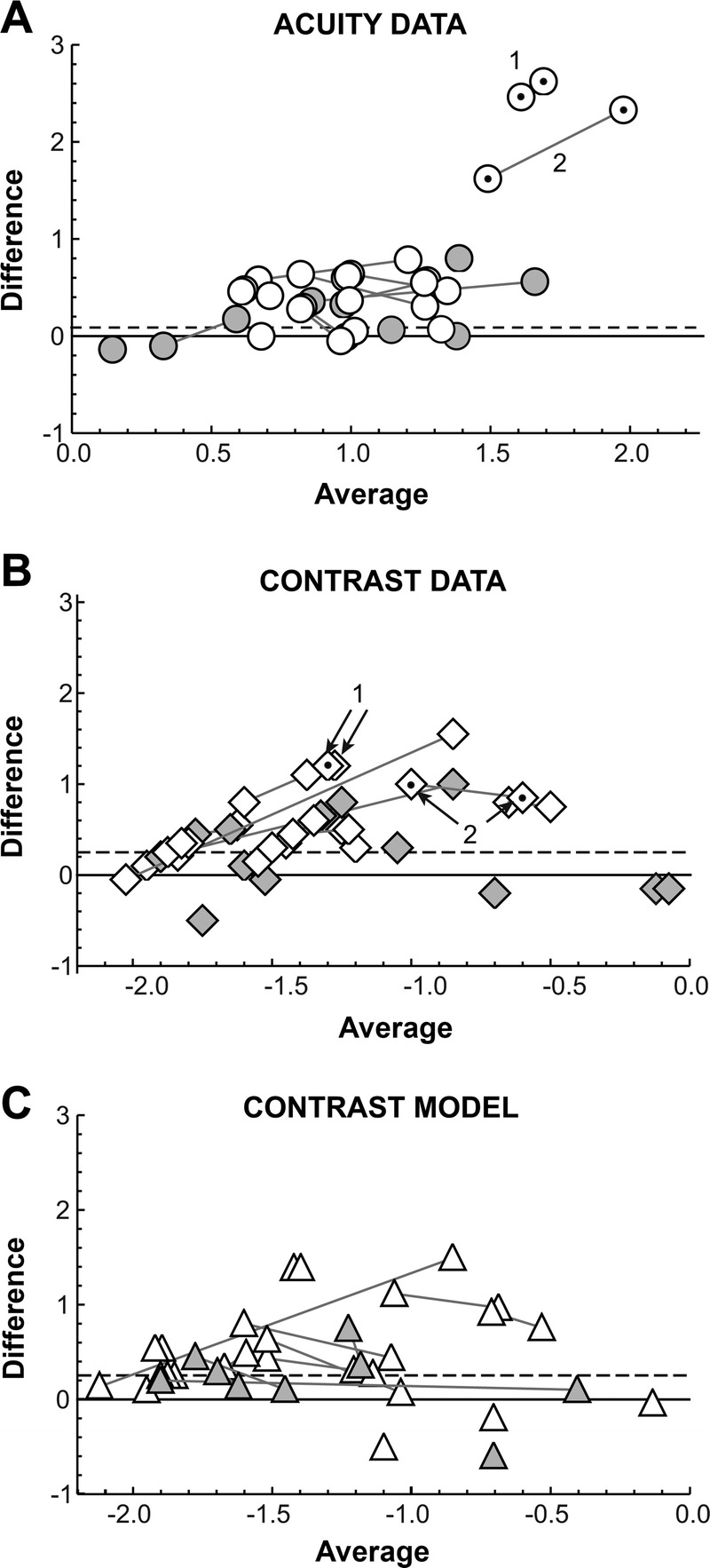
Results: Ohio Contrast Card contrast sensitivity was always less than 0.19 log10 units below the maximum possible contrast sensitivity predicted by the model; average Pelli-Robson letter contrast sensitivity was near the model prediction, but 0.516 log10 units below the maximum. Letter acuity was 0.336 logMAR below the grating acuity results. The model estimated the best testing distance in meters for optimum Pelli-Robson contrast sensitivity from the Bailey-Lovie acuity as distance = 1.5 - logMAR for low-vision patients. Of the four vision tests, only Ohio Contrast Card contrast sensitivity was independently and statistically significantly correlated with students' quality of life.
Conclusions: The Ohio Contrast Cards combine a grating stimulus, a looking indicator behavior, and contrast sensitivity measurement. They show promise for the clinical objective of advising the patient and his/her caregivers about the success the patient is likely to enjoy in tasks of everyday life.
Conflict of interest statement
Figures









References
-
- McDonald MA, Dobson V, Sebris SL, et al. The Acuity Card Procedure: A Rapid Test of Infant Acuity. Invest Ophthalmol Vis Sci 1985;26:1158–62. - PubMed
-
- Lennie P, Van Hemel SB. Visual Impairments: Determining Eligibility for Social Security Benefits. Washington, DC: National Academy Press; 2002. - PubMed
-
- Pelli D, Robson J, Wilkins A. The Design of a New Letter Chart for Measuring Contrast Sensitivity. Clin Vis Sci 1988;2:187–99.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
