

Potential discrepancy between plain films and CT scans in Brooker classification of heterotopic ossification
- PMID: 28972793
- PMCID: PMC6047644
- DOI: 10.1259/bjr.20170263
Potential discrepancy between plain films and CT scans in Brooker classification of heterotopic ossification
Abstract
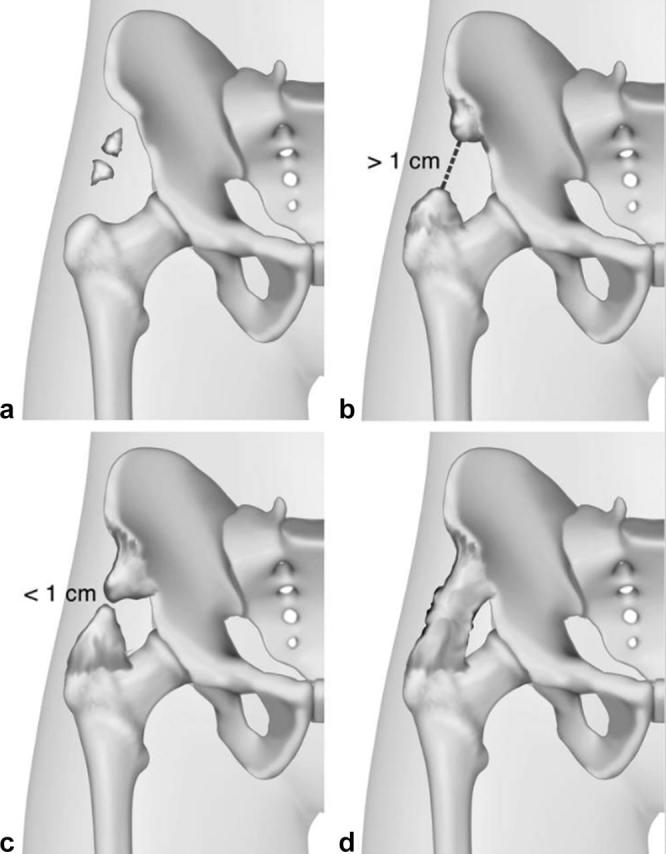
Objectives: The Brooker classification is a commonly used tool to characterize the extent of heterotopic ossification (HTO), which is the dystrophic formation of mature lamellar bone in non-osseous tissues such as muscles, connective tissue or nerves. We aim to provide illustrative cases to describe the limitations and challenges of this system.
Methods: A retrospective review was conducted in all patients who had retrieved hip and/or pelvic radiotherapy for HTO prophylaxis at Sunnybrook Health Sciences Centre between July 1998 and August 2016. An independent musculoskeletal radiologist who was blinded to the condition of the patient and the clinical outcome evaluated the imaging studies based on the Brooker classification.
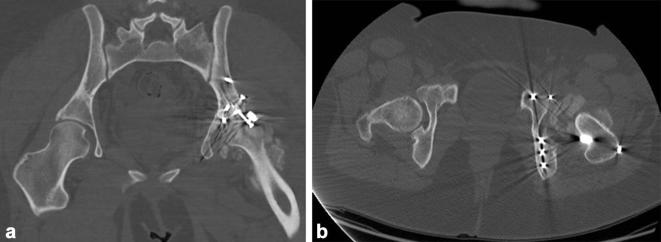
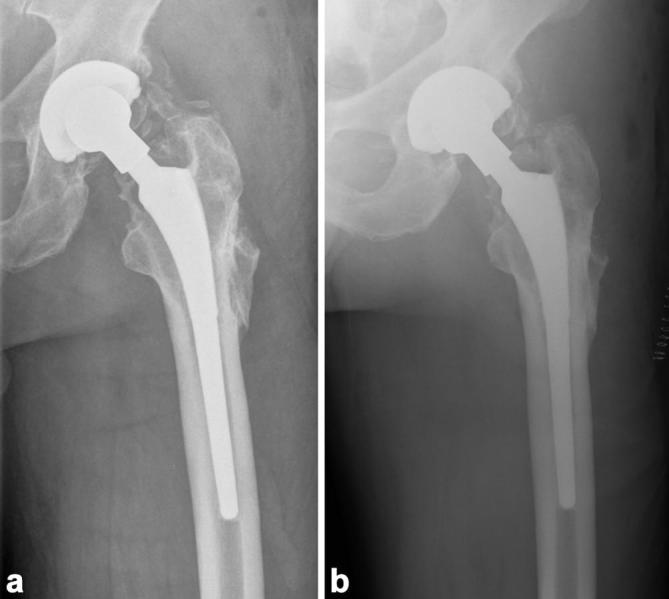
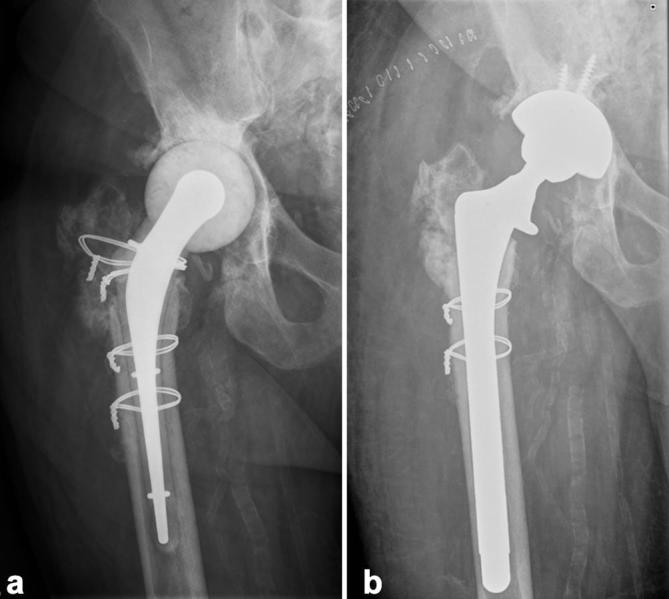
Results: 22 patients were identified for analysis. Three patient cases were presented to illustrate the discrepancies between the Brooker classification and radiographic images, CT images and different radiographical projections. Two patient cases were presented to demonstrate the inability of the Brooker classification to account for volumetric differences in HTO and arthroplasty lengths.
Conclusion: Although the Brooker classification for HTO is a widely used quantitative and qualitative assessment tool given its simplicity and familiarity, it possesses several limitations. Utilization of other radiographic modalities, such as CT, and orthogonal projections may reduce ambiguities from using the HTO system. Development of a classification method that can appropriately correspond to the clinical outcomes such as functional capabilities to further HTO development is warranted. Advances in knowledge: The present study critically evaluated the Brooker classification system, and identified areas in which improvement is warranted on characterizing HTO. This is important in further research that aims to improve the accuracy of HTO classification guidelines.
Keywords: Brooker Classification; Heterotopic ossification.
Figures




References
-
- Popovic M, Agarwal A, Zhang L, Yip C, Kreder HJ, Nousiainen MT, et al. Radiotherapy for the prophylaxis of heterotopic ossification: a systematic review and meta-analysis of published data. Radiother Oncol 2014; 113: 10–17. - PubMed
-
- Balboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006; 65: 1289–99. - PubMed
-
- Garland DE. A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res 1991; 263: 13–29. - PubMed
-
- Taussky D, Cserhati M, Pescia R. Preoperative radiotherapy without femoral shielding for prevention of heterotopic ossification in hydroxyapatite-coated hip prostheses. Arch Orthop Trauma Surg 2001; 121: 271–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
