

Gabapentin, opioids, and the risk of opioid-related death: A population-based nested case-control study
- PMID: 28972983
- PMCID: PMC5626029
- DOI: 10.1371/journal.pmed.1002396
Gabapentin, opioids, and the risk of opioid-related death: A population-based nested case-control study
Abstract
Background: Prescription opioid use is highly associated with risk of opioid-related death, with 1 of every 550 chronic opioid users dying within approximately 2.5 years of their first opioid prescription. Although gabapentin is widely perceived as safe, drug-induced respiratory depression has been described when gabapentin is used alone or in combination with other medications. Because gabapentin and opioids are both commonly prescribed for pain, the likelihood of co-prescription is high. However, no published studies have examined whether concomitant gabapentin therapy is associated with an increased risk of accidental opioid-related death in patients receiving opioids. The objective of this study was to investigate whether co-prescription of opioids and gabapentin is associated with an increased risk of accidental opioid-related mortality.
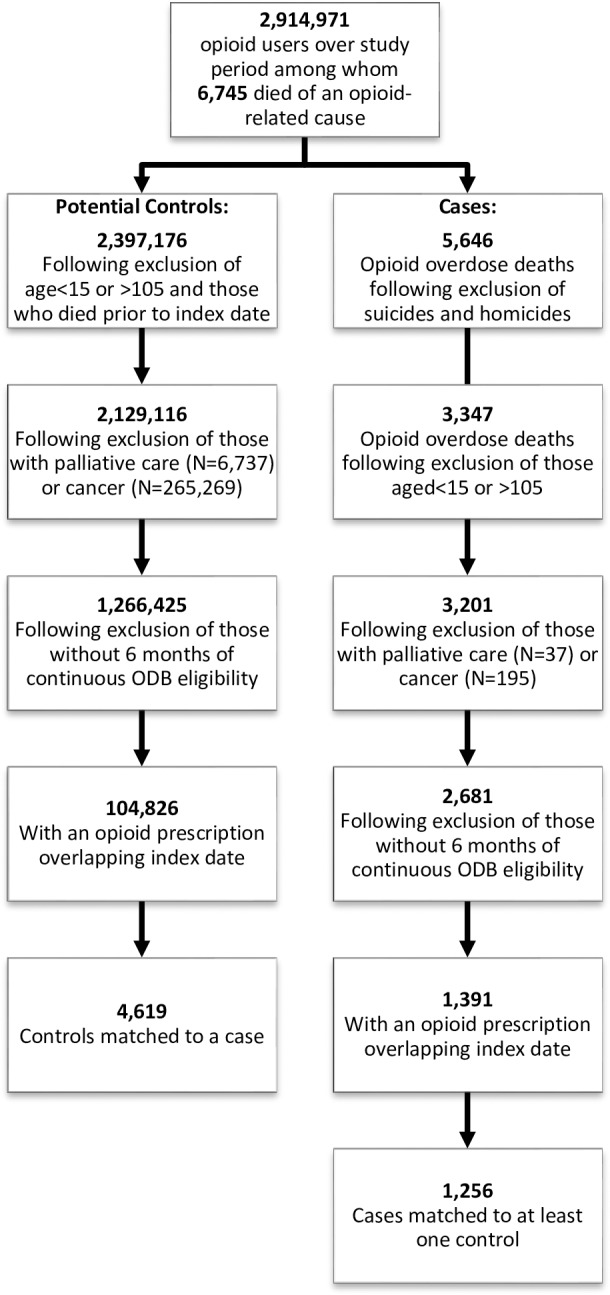
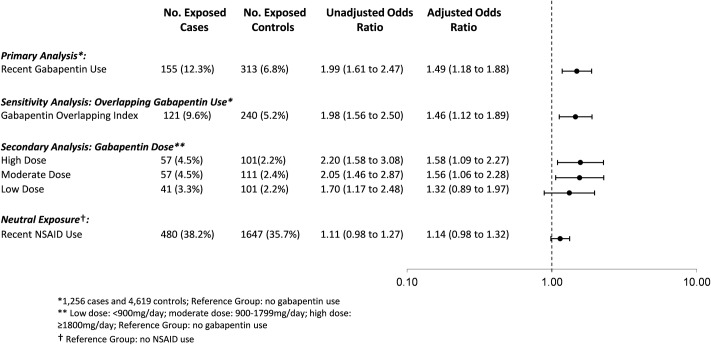
Methods and findings: We conducted a population-based nested case-control study among opioid users who were residents of Ontario, Canada, between August 1, 1997, and December 31, 2013, using administrative databases. Cases, defined as opioid users who died of an opioid-related cause, were matched with up to 4 controls who also used opioids on age, sex, year of index date, history of chronic kidney disease, and a disease risk index. After matching, we included 1,256 cases and 4,619 controls. The primary exposure was concomitant gabapentin use in the 120 days preceding the index date. A secondary analysis characterized gabapentin dose as low (<900 mg daily), moderate (900 to 1,799 mg daily), or high (≥1,800 mg daily). A sensitivity analysis examined the effect of concomitant nonsteroidal anti-inflammatory drug (NSAID) use in the preceding 120 days. Overall, 12.3% of cases (155 of 1,256) and 6.8% of controls (313 of 4,619) were prescribed gabapentin in the prior 120 days. After multivariable adjustment, co-prescription of opioids and gabapentin was associated with a significantly increased odds of opioid-related death (odds ratio [OR] 1.99, 95% CI 1.61 to 2.47, p < 0.001; adjusted OR [aOR] 1.49, 95% CI 1.18 to 1.88, p < 0.001) compared to opioid prescription alone. In the dose-response analysis, moderate-dose (OR 2.05, 95% CI 1.46 to 2.87, p < 0.001; aOR 1.56, 95% CI 1.06 to 2.28, p = 0.024) and high-dose (OR 2.20, 95% CI 1.58 to 3.08, p < 0.001; aOR 1.58, 95% CI 1.09 to 2.27, p = 0.015) gabapentin use was associated with a nearly 60% increase in the odds of opioid-related death relative to no concomitant gabapentin use. As expected, we found no significant association between co-prescription of opioids and NSAIDs and opioid-related death (OR 1.11, 95% CI 0.98 to 1.27, p = 0.113; aOR 1.14, 95% CI 0.98 to 1.32, p = 0.083). In an exploratory analysis of patients at risk of combined opioid and gabapentin use, we found that 46.0% (45,173 of 98,288) of gabapentin users in calendar year 2013 received at least 1 concomitant prescription for an opioid. This study was limited to individuals eligible for public drug coverage in Ontario, we were only able to identify prescriptions reimbursed by the government and dispensed from retail pharmacies, and information on indication for gabapentin use was not available. Furthermore, as with all observational studies, confounding due to unmeasured variables is a potential source of bias.
Conclusions: In this study we found that among patients receiving prescription opioids, concomitant treatment with gabapentin was associated with a substantial increase in the risk of opioid-related death. Clinicians should consider carefully whether to continue prescribing this combination of products and, when the combination is deemed necessary, should closely monitor their patients and adjust opioid dose accordingly. Future research should investigate whether a similar interaction exists between pregabalin and opioids.
Conflict of interest statement
TA is supported by a New Investigator Award from the Canadian Institutes for Health Research (CIHR). DNJ has provided expert opinion on medicolegal matters, some of which have involved opioids (in no instances has DNJ engaged in paid work for or against opioid manufacturers.) Income received from speaking or expert testimony is tithed by The Sunnybrook Department of Medicine as part of their academic practice plan. MMM has served on advisory boards and reports honoraria from Bristol-Myers Squibb, Eli Lilly and Company, Glaxo Smith Kline, Hoffman La Roche, Novartis, Novo Nordisk, Pfizer, and Astra Zeneca, all outside the submitted work. WvdB received honoraria from Lundbeck, Indivior, Mundipharma, Novartis, Bioproject, Eli Lilly and Pfizer. All other authors report no conflicts of interest.
Figures
References
-
- US Centers for Disease Control and Prevention. Prescription opioid overdose data. Atlanta: US Centers for Disease Control and Prevention; 2017. [cited 2017 Sep 5]. Available from: http://www.cdc.gov/drugoverdose/data/overdose.html.
-
- Park TW, Saitz R, Ganoczy D, Ilgen MA, Bohnert AS. Benzodiazepine prescribing patterns and deaths from drug overdose among US veterans receiving opioid analgesics: case-cohort study. BMJ. 2015;350:h2698 doi: 10.1136/bmj.h2698 - DOI - PMC - PubMed
-
- US Food and Drug Administration. New safety measures announced for opioid analgesics, prescription opioid cough products, and benzodiazepines. Silver Spring (Maryland): US Food and Drug Administration; 2016. August 31 [cited 2017 Aug 30]. Available from: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm518110.htm.
-
- Kaplovitch E, Gomes T, Camacho X, Dhalla IA, Mamdani MM, Juurlink DN. Sex differences in dose escalation and overdose death during chronic opioid therapy: a population-based cohort study. PLoS ONE. 2015;10(8):e0134550 doi: 10.1371/journal.pone.0134550 - DOI - PMC - PubMed
-
- Bockbrader HN, Wesche D, Miller R, Chapel S, Janiczek N, Burger P. A comparison of the pharmacokinetics and pharmacodynamics of pregabalin and gabapentin. Clin Pharmacokinet. 2010;49(10):661–9. doi: 10.2165/11536200-000000000-00000 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
