

Effect of Systematic Intensive Care Unit Triage on Long-term Mortality Among Critically Ill Elderly Patients in France: A Randomized Clinical Trial
- PMID: 28973065
- PMCID: PMC5710364
- DOI: 10.1001/jama.2017.13889
Effect of Systematic Intensive Care Unit Triage on Long-term Mortality Among Critically Ill Elderly Patients in France: A Randomized Clinical Trial
Abstract
Importance: The high mortality rate in critically ill elderly patients has led to questioning of the beneficial effect of intensive care unit (ICU) admission and to a variable ICU use among this population.
Objective: To determine whether a recommendation for systematic ICU admission in critically ill elderly patients reduces 6-month mortality compared with usual practice.
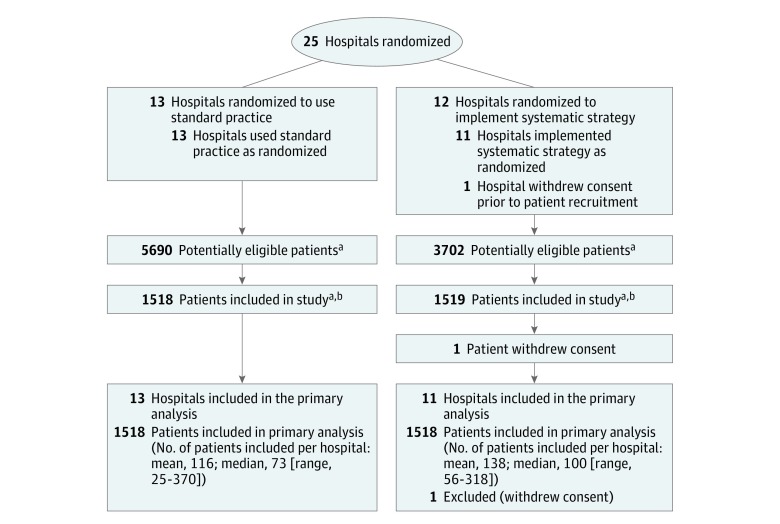
Design, setting, and participants: Multicenter, cluster-randomized clinical trial of 3037 critically ill patients aged 75 years or older, free of cancer, with preserved functional status (Index of Independence in Activities of Daily Living ≥4) and nutritional status (absence of cachexia) who arrived at the emergency department of one of 24 hospitals in France between January 2012 and April 2015 and were followed up until November 2015.
Interventions: Centers were randomly assigned either to use a program to promote systematic ICU admission of patients (n=1519 participants) or to follow standard practice (n=1518 participants).
Main outcomes and measures: The primary outcome was death at 6 months. Secondary outcomes included ICU admission rate, in-hospital death, functional status, and quality of life (12-Item Short Form Health Survey, ranging from 0 to 100, with higher score representing better self-reported health) at 6 months.
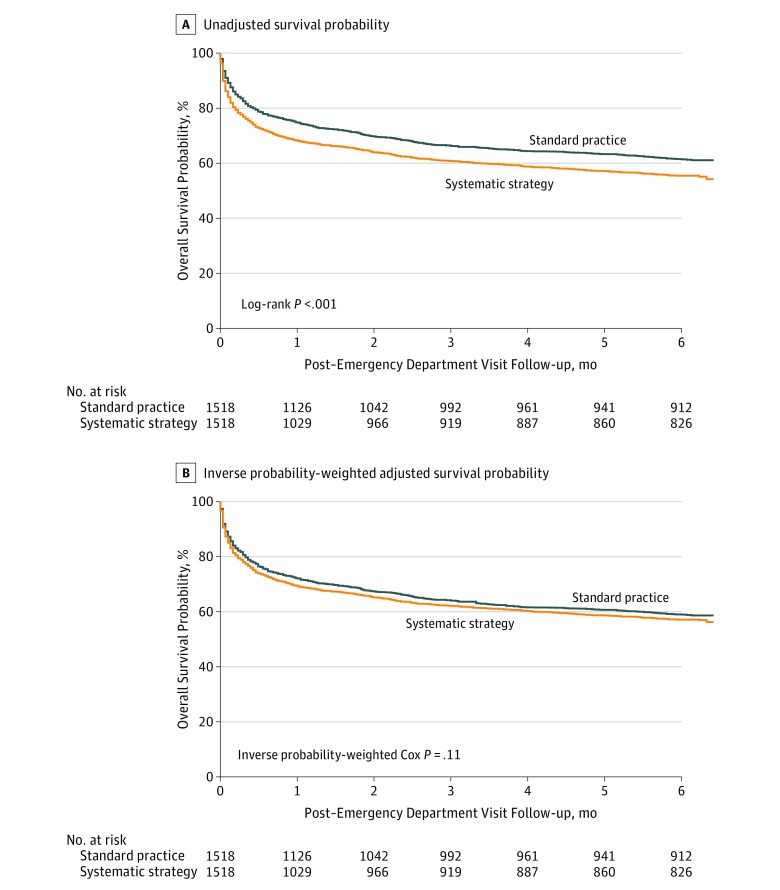
Results: One patient withdrew consent, leaving 3036 patients included in the trial (median age, 85 [interquartile range, 81-89] years; 1361 [45%] men). Patients in the systematic strategy group had an increased risk of death at 6 months (45% vs 39%; relative risk [RR], 1.16; 95% CI, 1.07-1.26) despite an increased ICU admission rate (61% vs 34%; RR, 1.80; 95% CI, 1.66-1.95). After adjustments for baseline characteristics, patients in the systematic strategy group were more likely to be admitted to an ICU (RR, 1.68; 95% CI, 1.54-1.82) and had a higher risk of in-hospital death (RR, 1.18; 95% CI, 1.03-1.33) but had no significant increase in risk of death at 6 months (RR, 1.05; 95% CI, 0.96-1.14). Functional status and physical quality of life at 6 months were not significantly different between groups.
Conclusions and relevance: Among critically ill elderly patients in France, a program to promote systematic ICU admission increased ICU use but did not reduce 6-month mortality. Additional research is needed to understand the decision to admit elderly patients to the ICU.
Trial registration: clinicaltrials.gov Identifier: NCT01508819.
Conflict of interest statement
Figures
Comment in
-
Admitting Elderly Patients to the Intensive Care Unit-Is it the Right Decision?JAMA. 2017 Oct 17;318(15):1443-1444. doi: 10.1001/jama.2017.14535. JAMA. 2017. PMID: 28973429 No abstract available.
-
ICU Admission and Mortality Among Elderly Adults.JAMA. 2018 Mar 13;319(10):1047. doi: 10.1001/jama.2017.21668. JAMA. 2018. PMID: 29536090 No abstract available.
References
-
- Flaatten H, de Lange DW, Artigas A, et al. The status of intensive care medicine research and a future agenda for very old patients in the ICU. Intensive Care Med. 2017;43(9):1319-1328. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
