

Association of Paravalvular Regurgitation With 1-Year Outcomes After Transcatheter Aortic Valve Replacement With the SAPIEN 3 Valve
- PMID: 28973091
- PMCID: PMC5710359
- DOI: 10.1001/jamacardio.2017.3425
Association of Paravalvular Regurgitation With 1-Year Outcomes After Transcatheter Aortic Valve Replacement With the SAPIEN 3 Valve
Abstract
Importance: Moderate/severe and even mild paravalvular regurgitation (PVR) are associated with increased mortality following transcatheter aortic valve replacement (TAVR) with first and second generations of transcatheter valves.
Objective: To examine the incidence, evolution, and effect on 1-year outcomes of PVR following TAVR with a third-generation balloon-expandable transcatheter heart valve.
Design, setting, and participants: Prespecified analysis of PVR in the Placement of Aortic Transcatheter Valves (PARTNER) II SAPIEN 3 trial, conducted between October 1, 2013, and September 3, 2014. Multicenter, nonrandomized registry of 1661 patients at intermediate or high surgical risk undergoing TAVR with the SAPIEN 3. Patients with severe, symptomatic aortic stenosis and high/intermediate surgical risk were enrolled in the registry at 51 sites in the United States and Canada.
Interventions: Transcatheter aortic valve replacement with the SAPIEN 3 valve.
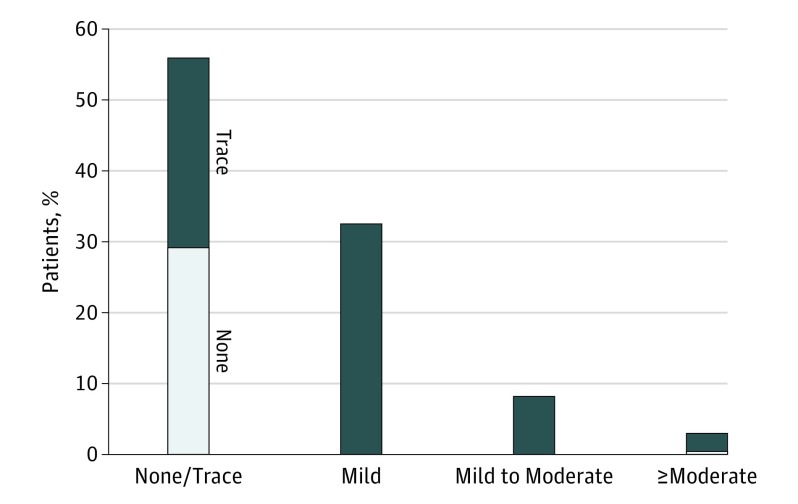
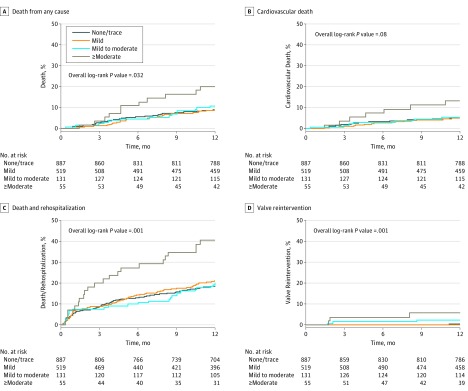
Main outcomes and measures: Paravalvular regurgitation was assessed in a core laboratory at 30 days and 1 year according to a 5-class scheme: 0, none or trace; 1, mild; 2, mild to moderate; 3, moderate; 4, moderate to severe; and 5, severe. We assessed the effect of PVR on 1-year mortality and heart failure rehospitalization.
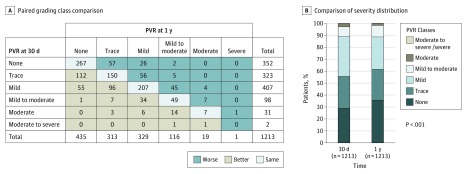
Results: Among the 1661 included in the registry, 1592 received a SAPIEN 3 valve and had assessment of PVR. Of these patients, 55.7% had none-trace PVR, 32.6% had mild, 8.2% had mild to moderate, and 3.5% had at least moderate PVR at 30 days. At 1 year, 9.3% of patients had died and 14.2% had been rehospitalized. Only patients with at least moderate PVR had higher 1-year mortality (hazard ratio [HR], 2.40; 95% CI, 1.30-4.43; P = .005) and composite of mortality/rehospitalization (HR, 2.35; 95% CI, 1.52-3.62; P < .001). In a paired comparison including 1213 patients, 73% of the patients with at least moderate PVR at 30 days showed a reduction in PVR severity of at least 1 PVR class at 1 year.
Conclusions and relevance: In this series of patients undergoing TAVR with the SAPIEN 3 valve, at least moderate PVR was rare but associated with increased risk of death and heart failure rehospitalization at 1 year. Even the upper range of the mild class in the 3-class grading scheme (ie, mild to moderate in the 5-class scheme) had no significant effect on short-term mortality or rehospitalization. Most patients with at least moderate PVR at 30 days showed a decrease of PVR severity grade at 1 year.
Trial registration: clinicaltrials.gov Identifier: NCT01314313.
Conflict of interest statement
Figures
References
-
- Leon MB, Smith CR, Mack M, et al. ; PARTNER Trial Investigators . Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607. - PubMed
-
- Kodali SK, Williams MR, Smith CR, et al. ; PARTNER Trial Investigators . Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366(18):1686-1695. - PubMed
-
- Adams DH, Popma JJ, Reardon MJ, et al. ; U.S. CoreValve Clinical Investigators . Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370(19):1790-1798. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57-e185. - PubMed
-
- Leon MB, Smith CR, Mack MJ, et al. ; PARTNER 2 Investigators . Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374(17):1609-1620. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
