

Defining Optimal Length of Opioid Pain Medication Prescription After Common Surgical Procedures
- PMID: 28973092
- PMCID: PMC5833616
- DOI: 10.1001/jamasurg.2017.3132
Defining Optimal Length of Opioid Pain Medication Prescription After Common Surgical Procedures
Abstract
Importance: The overprescription of pain medications has been implicated as a driver of the burgeoning opioid epidemic; however, few guidelines exist regarding the appropriateness of opioid pain medication prescriptions after surgery.
Objectives: To describe patterns of opioid pain medication prescriptions after common surgical procedures and determine the appropriateness of the prescription as indicated by the rate of refills.
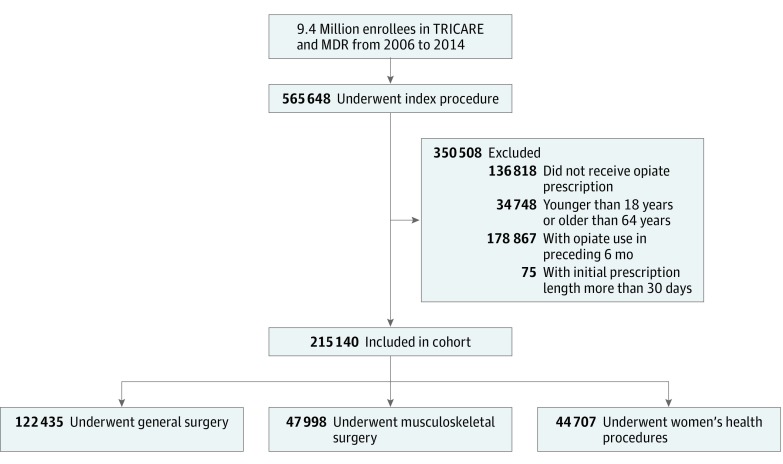
Design, setting, and participants: The Department of Defense Military Health System Data Repository was used to identify opioid-naive individuals 18 to 64 years of age who had undergone 1 of 8 common surgical procedures between January 1, 2005, and September 30, 2014. The adjusted risk of refilling an opioid prescription based on the number of days of initial prescription was modeled using a generalized additive model with spline smoothing.
Exposures: Length of initial prescription for opioid pain medication.
Main outcomes and measures: Need for an additional subsequent prescription for opioid pain medication, or a refill.
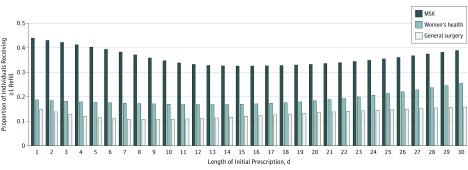
Results: Of the 215 140 individuals (107 588 women and 107 552 men; mean [SD] age, 40.1 [12.8] years) who underwent a procedure within the study time frame and received and filled at least 1 prescription for opioid pain medication within 14 days of their index procedure, 41 107 (19.1%) received at least 1 refill prescription. The median prescription lengths were 4 days (interquartile range [IQR], 3-5 days) for appendectomy and cholecystectomy, 5 days (IQR, 3-6 days) for inguinal hernia repair, 4 days (IQR, 3-5 days) for hysterectomy, 5 days (IQR, 3-6 days) for mastectomy, 5 days (IQR, 4-8 days) for anterior cruciate ligament repair and rotator cuff repair, and 7 days (IQR, 5-10 days) for discectomy. The early nadir in the probability of refill was at an initial prescription of 9 days for general surgery procedures (probability of refill, 10.7%), 13 days for women's health procedures (probability of refill, 16.8%), and 15 days for musculoskeletal procedures (probability of refill, 32.5%).
Conclusions and relevance: Ideally, opioid prescriptions after surgery should balance adequate pain management against the duration of treatment. In practice, the optimal length of opioid prescriptions lies between the observed median prescription length and the early nadir, or 4 to 9 days for general surgery procedures, 4 to 13 days for women's health procedures, and 6 to 15 days for musculoskeletal procedures.
Conflict of interest statement
Figures
Comment in
-
Addressing Variability in Opioid Prescribing.JAMA Surg. 2018 Jan 1;153(1):43. doi: 10.1001/jamasurg.2017.3166. JAMA Surg. 2018. PMID: 28973361 No abstract available.
-
Defining Postoperative Opioid Needs Among Preoperative Opioid Users.JAMA Surg. 2018 Jul 1;153(7):689-690. doi: 10.1001/jamasurg.2018.0217. JAMA Surg. 2018. PMID: 29590286 No abstract available.
-
Defining Postoperative Opioid Needs Among Preoperative Opioid Users-Reply.JAMA Surg. 2018 Jul 1;153(7):690. doi: 10.1001/jamasurg.2018.0218. JAMA Surg. 2018. PMID: 29590319 No abstract available.
References
-
- Dart RC, Surratt HL, Cicero TJ, et al. Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015;372(3):241-248. - PubMed
-
- Hill MV, McMahon ML, Stucke RS, Barth RJ Jr. Wide variation and excessive dosage of opioid prescriptions for common general surgical procedures. Ann Surg. 2017;265(4):709-714. - PubMed
-
- Paulozzi LJ, Mack KA, Hockenberry JM; Division of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC . Vital signs: variation among states in prescribing of opioid pain relievers and benzodiazepines—United States, 2012. MMWR Morb Mortal Wkly Rep. 2014;63(26):563-568. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
