

Association of Pathologic Nodal Staging Quality With Survival Among Patients With Non-Small Cell Lung Cancer After Resection With Curative Intent
- PMID: 28973110
- PMCID: PMC5833630
- DOI: 10.1001/jamaoncol.2017.2993
Association of Pathologic Nodal Staging Quality With Survival Among Patients With Non-Small Cell Lung Cancer After Resection With Curative Intent
Abstract
Importance: Pathologic nodal stage is the most significant prognostic factor in resectable non-small cell lung cancer (NSCLC). The International Association for the Study of Lung Cancer NSCLC staging project revealed intercontinental differences in N category-stratified survival. These differences may indicate differences not only in cancer biology but also in the thoroughness of the nodal examination.
Objective: To determine whether survival was affected by sequentially more stringent definitions of pN staging quality in a cohort of patients with NSCLC after resection with curative intent.
Design: This observational study used the Mid-South Quality of Surgical Resection cohort, a population-based database of lung cancer resections with curative intent. A total of 2047 consecutive patients who underwent surgical resection at 11 hospitals with at least 5 annual lung cancer resections in 4 contiguous US Dartmouth hospital referral regions in northern Mississippi, eastern Arkansas, and western Tennessee (>90% of the eligible population) were included. Resections were performed from January 1, 2009, through January 25, 2016. Survival was evaluated with the Kaplan-Meier method and Cox proportional hazards models.
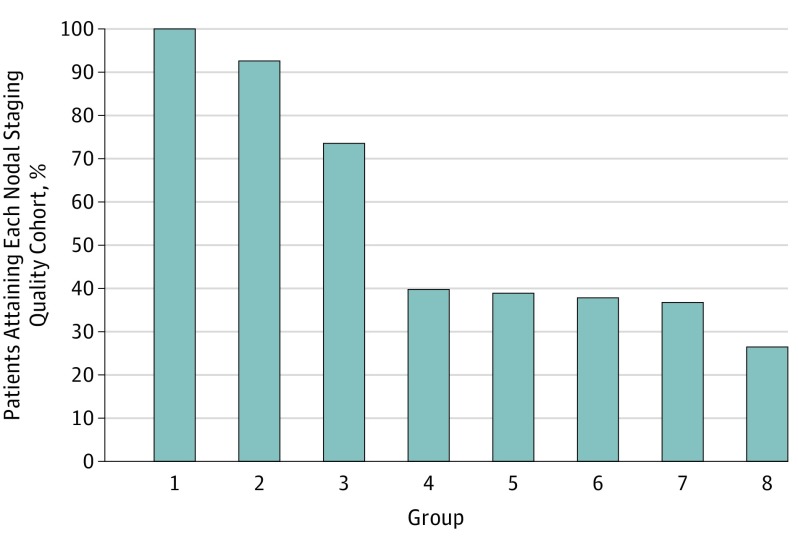
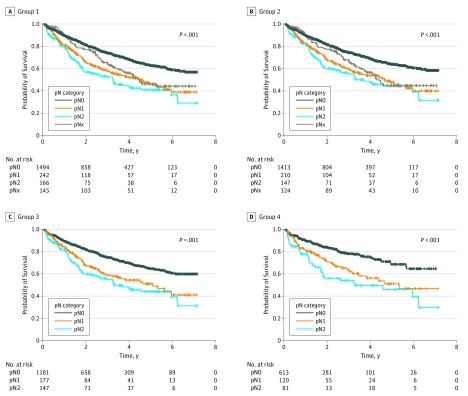
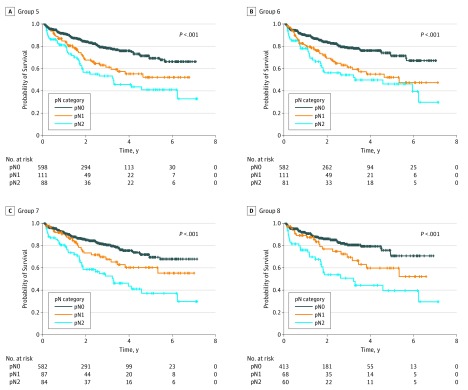
Exposures: Eight sequentially more stringent pN staging quality strata included the following: all patients (group 1); those with complete resections only (group 2); those with examination of at least 1 mediastinal lymph node (group 3); those with examination of at least 10 lymph nodes (group 4); those with examination of at least 3 hilar or intrapulmonary and at least 3 mediastinal lymph nodes (group 5); those with examination of at least 10 lymph nodes, including at least 1 mediastinal lymph node (group 6); those with examination of at least 1 hilar or intrapulmonary and at least 3 mediastinal nodal stations (group 7); and those with examination of at least 1 hilar or intrapulmonary lymph node, at least 10 total lymph nodes, and at least 3 mediastinal nodal stations (group 8).
Main outcomes and measures: N category-stratified overall survival.
Results: Of the total 2047 patients (1046 men [51.1%] and 1001 women [48.9%]; mean [SD] age, 67.0 [9.6] years) included in the analysis, the eligible analysis population ranged from 541 to 2047, depending on stringency. Sequential improvement in the N category-stratified 5-year survival of pN0 and pN1 tumors was found from the least stringent group (0.63 [95% CI, 0.59-0.66] for pN0 vs 0.46 [95% CI, 0.38-0.54] for pN1) to the most stringent group (0.71 [95% CI, 0.60-0.79] for pN0 vs 0.60 [95% CI, 0.43-0.73] for pN1). The pN1 cohorts with 3 or more mediastinal nodal stations examined had the most striking survival improvements. More stringently defined mediastinal nodal examination was associated with better separation in survival curves between patients with pN1 and pN2 tumors.
Conclusions and relevance: The prognostic value of pN stratification depends on the thoroughness of examination. Differences in thoroughness of nodal staging may explain a large proportion of intercontinental survival differences. More thorough nodal examination practice must be disseminated to improve the prognostic value of the TNM staging system. Future updates of the TNM staging system should incorporate more quality restraints.
Conflict of interest statement
Figures
Comment in
-
Quality of Lymph Node Assessment and Survival Among Patients With Non-Small Cell Lung Cancer.JAMA Oncol. 2018 Jan 1;4(1):1-2. doi: 10.1001/jamaoncol.2017.3092. JAMA Oncol. 2018. PMID: 28973558 No abstract available.
References
-
- Goldstraw P, Chansky K, Crowley J, et al. ; International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions; International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee advisory boards and participating institutions . The IASLC Lung Cancer Staging Project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):39-51. - PubMed
-
- Osarogiagbon RU, Allen JW, Farooq A, Wu JT. Objective review of mediastinal lymph node examination in a lung cancer resection cohort. J Thorac Oncol. 2012;7(2):390-396. - PubMed
-
- Detterbeck FC. The fable of Babel and building a foundation for quality. J Thorac Oncol. 2012;7(2):267-268. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
