

Effect of an Early Resuscitation Protocol on In-hospital Mortality Among Adults With Sepsis and Hypotension: A Randomized Clinical Trial
- PMID: 28973227
- PMCID: PMC5710318
- DOI: 10.1001/jama.2017.10913
Effect of an Early Resuscitation Protocol on In-hospital Mortality Among Adults With Sepsis and Hypotension: A Randomized Clinical Trial
Abstract
Importance: The effect of an early resuscitation protocol on sepsis outcomes in developing countries remains unknown.
Objective: To determine whether an early resuscitation protocol with administration of intravenous fluids, vasopressors, and blood transfusion decreases mortality among Zambian adults with sepsis and hypotension compared with usual care.
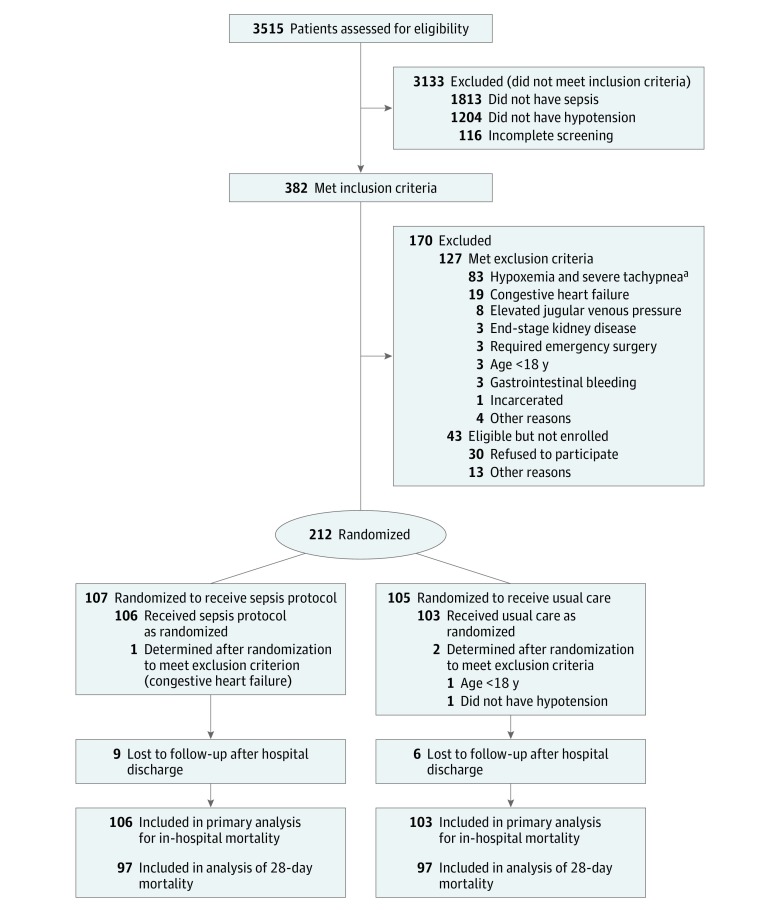
Design, setting, and participants: Randomized clinical trial of 212 adults with sepsis (suspected infection plus ≥2 systemic inflammatory response syndrome criteria) and hypotension (systolic blood pressure ≤90 mm Hg or mean arterial pressure ≤65 mm Hg) presenting to the emergency department at a 1500-bed referral hospital in Zambia between October 22, 2012, and November 11, 2013. Data collection concluded December 9, 2013.
Interventions: Patients were randomized 1:1 to either (1) an early resuscitation protocol for sepsis (n = 107) that included intravenous fluid bolus administration with monitoring of jugular venous pressure, respiratory rate, and arterial oxygen saturation and treatment with vasopressors targeting mean arterial pressure (≥65 mm Hg) and blood transfusion (for patients with a hemoglobin level <7 g/dL) or (2) usual care (n = 105) in which treating clinicians determined hemodynamic management.
Main outcomes and measures: The primary outcome was in-hospital mortality and the secondary outcomes included the volume of intravenous fluid received and receipt of vasopressors.
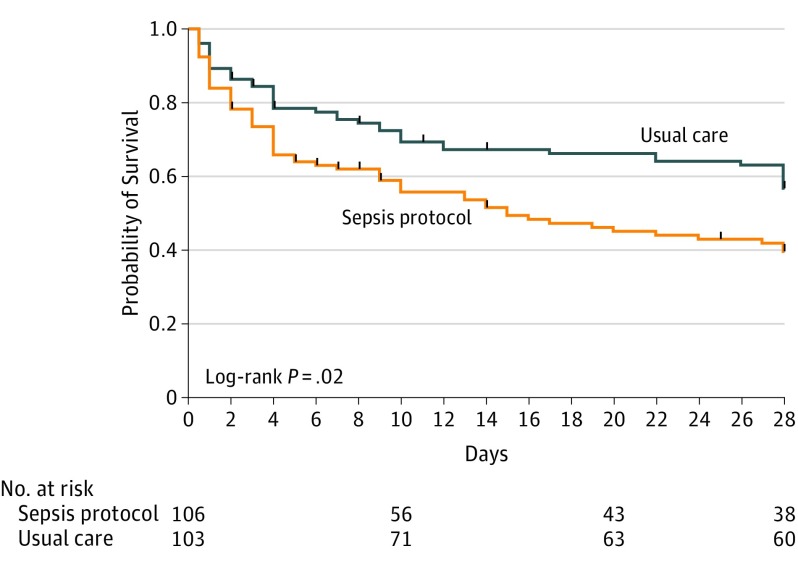
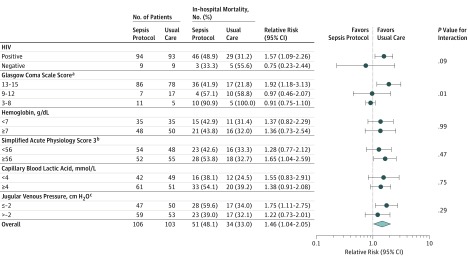
Results: Among 212 patients randomized to receive either the sepsis protocol or usual care, 3 were ineligible and the remaining 209 completed the study and were included in the analysis (mean [SD] age, 36.7 [12.4] years; 117 men [56.0%]; 187 [89.5%] positive for the human immunodeficiency virus). The primary outcome of in-hospital mortality occurred in 51 of 106 patients (48.1%) in the sepsis protocol group compared with 34 of 103 patients (33.0%) in the usual care group (between-group difference, 15.1% [95% CI, 2.0%-28.3%]; relative risk, 1.46 [95% CI, 1.04-2.05]; P = .03). In the 6 hours after presentation to the emergency department, patients in the sepsis protocol group received a median of 3.5 L (interquartile range, 2.7-4.0 L) of intravenous fluid compared with 2.0 L (interquartile range, 1.0-2.5 L) in the usual care group (mean difference, 1.2 L [95% CI, 1.0-1.5 L]; P < .001). Fifteen patients (14.2%) in the sepsis protocol group and 2 patients (1.9%) in the usual care group received vasopressors (between-group difference, 12.3% [95% CI, 5.1%-19.4%]; P < .001).
Conclusions and relevance: Among adults with sepsis and hypotension, most of whom were positive for HIV, in a resource-limited setting, a protocol for early resuscitation with administration of intravenous fluids and vasopressors increased in-hospital mortality compared with usual care. Further studies are needed to understand the effects of administration of intravenous fluid boluses and vasopressors in patients with sepsis across different low- and middle-income clinical settings and patient populations.
Trial registration: clinicaltrials.gov Identifier: NCT01663701.
Conflict of interest statement
Figures
Comment in
-
Trying to Improve Sepsis Care in Low-Resource Settings.JAMA. 2017 Oct 3;318(13):1225-1227. doi: 10.1001/jama.2017.10547. JAMA. 2017. PMID: 28973226 No abstract available.
-
The forgotten value of the clinical examination to individualize and guide fluid resuscitation in patients with sepsis.Crit Care. 2017 Dec 19;21(1):306. doi: 10.1186/s13054-017-1898-4. Crit Care. 2017. PMID: 29258571 Free PMC article. No abstract available.
-
Early Resuscitation for Adults With Sepsis in a Low-Income Country.JAMA. 2018 Feb 13;319(6):614. doi: 10.1001/jama.2017.20406. JAMA. 2018. PMID: 29450518 No abstract available.
-
Decision-making in the detection and management of patients with sepsis in resource-limited settings: the importance of clinical examination.Crit Care. 2018 Mar 1;22(1):53. doi: 10.1186/s13054-018-1971-7. Crit Care. 2018. PMID: 29490677 Free PMC article. No abstract available.
Similar articles
-
REstricted Fluid REsuscitation in Sepsis-associated Hypotension (REFRESH): study protocol for a pilot randomised controlled trial.Trials. 2017 Aug 29;18(1):399. doi: 10.1186/s13063-017-2137-7. Trials. 2017. PMID: 28851407 Free PMC article. Clinical Trial.
-
Restricted fluid resuscitation in suspected sepsis associated hypotension (REFRESH): a pilot randomised controlled trial.Intensive Care Med. 2018 Dec;44(12):2070-2078. doi: 10.1007/s00134-018-5433-0. Epub 2018 Oct 31. Intensive Care Med. 2018. PMID: 30382308 Clinical Trial.
-
A randomized trial of protocol-based care for early septic shock.N Engl J Med. 2014 May 1;370(18):1683-93. doi: 10.1056/NEJMoa1401602. Epub 2014 Mar 18. N Engl J Med. 2014. PMID: 24635773 Free PMC article. Clinical Trial.
-
Fluid Therapy for Critically Ill Adults With Sepsis: A Review.JAMA. 2023 Jun 13;329(22):1967-1980. doi: 10.1001/jama.2023.7560. JAMA. 2023. PMID: 37314271 Review.
-
The initial resuscitation of septic shock.J Crit Care. 2020 Jun;57:108-117. doi: 10.1016/j.jcrc.2020.02.004. Epub 2020 Feb 11. J Crit Care. 2020. PMID: 32135409 Review.
Cited by
-
COVID-19 medical management including World Health Organization (WHO) suggested management strategies.Dis Mon. 2020 Sep;66(9):101068. doi: 10.1016/j.disamonth.2020.101068. Epub 2020 Aug 28. Dis Mon. 2020. PMID: 32907701 Free PMC article. Review. No abstract available.
-
Fluid Therapy and the Microcirculation in Health and Critical Illness.Front Vet Sci. 2021 May 13;8:625708. doi: 10.3389/fvets.2021.625708. eCollection 2021. Front Vet Sci. 2021. PMID: 34055944 Free PMC article. Review.
-
Association of fluid balance with mortality in sepsis is modified by admission hemoglobin levels: A large database study.PLoS One. 2021 Jun 14;16(6):e0252629. doi: 10.1371/journal.pone.0252629. eCollection 2021. PLoS One. 2021. PMID: 34125858 Free PMC article.
-
Early management of sepsis in medical patients in rural Thailand: a single-center prospective observational study.J Intensive Care. 2019 Dec 2;7:55. doi: 10.1186/s40560-019-0407-z. eCollection 2019. J Intensive Care. 2019. PMID: 31827803 Free PMC article.
-
Focus on sepsis: new concepts and findings in sepsis care.Intensive Care Med. 2018 Nov;44(11):1997-1999. doi: 10.1007/s00134-018-5406-3. Epub 2018 Oct 10. Intensive Care Med. 2018. PMID: 30306194 No abstract available.
References
-
- Kaukonen K-M, Bailey M, Suzuki S, et al. . Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA. 2014;311(13):1308-1316. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. . Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-1377. - PubMed
-
- Levy MM, Rhodes A, Phillips GS, et al. . Surviving Sepsis Campaign. Crit Care Med. 2015;43(1):3-12. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
