

Correlation Between Macular Integrity Assessment and Optical Coherence Tomography Imaging of Ellipsoid Zone in Macular Telangiectasia Type 2
- PMID: 28973315
- PMCID: PMC6024664
- DOI: 10.1167/iovs.17-21834
Correlation Between Macular Integrity Assessment and Optical Coherence Tomography Imaging of Ellipsoid Zone in Macular Telangiectasia Type 2
Abstract
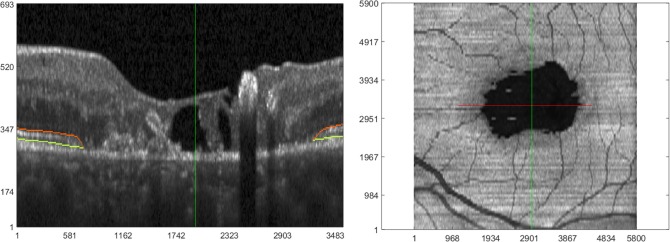
Purpose: To correlate ellipsoid zone (EZ) defects on spectral-domain optical coherence tomography (SD-OCT) with retinal sensitivity loss on macular integrity assessment (MAIA) microperimetry in macular telangiectasia type 2 (MacTel).
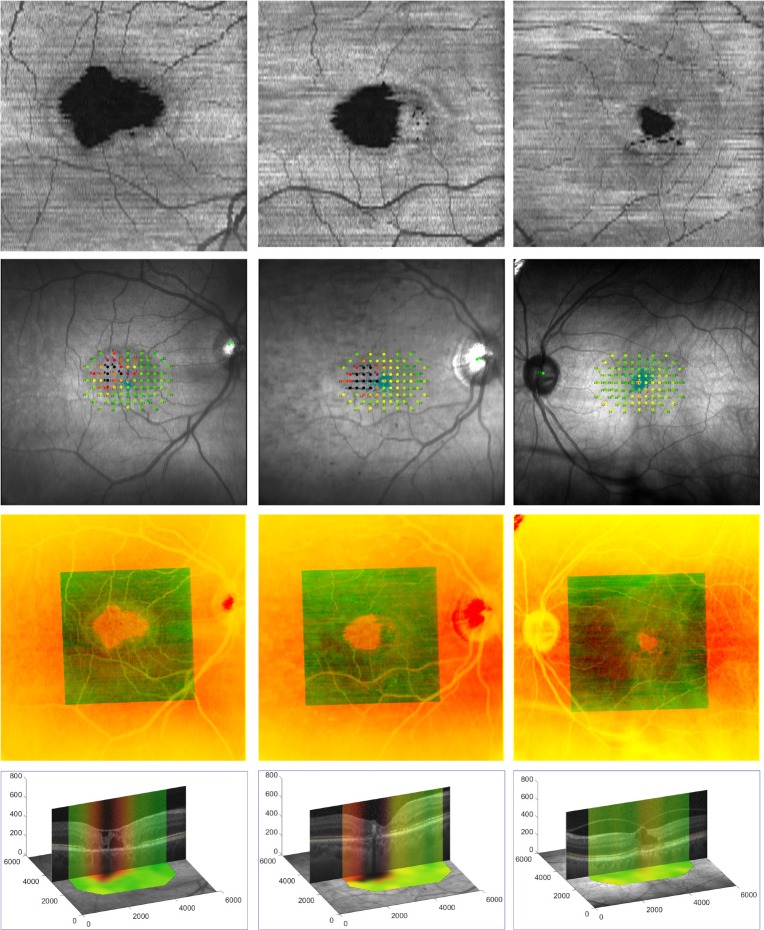
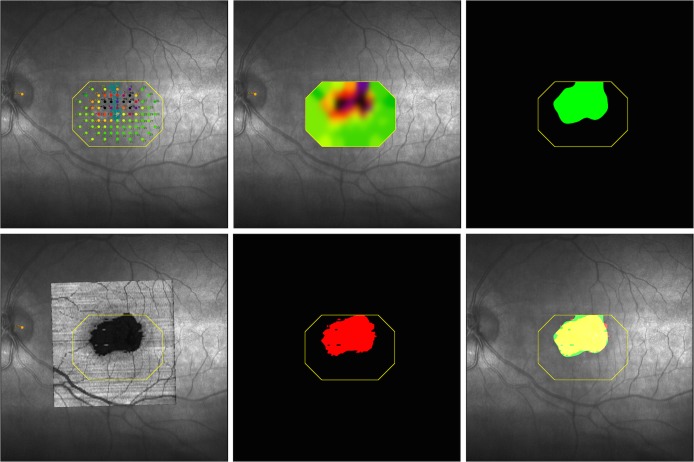
Methods: Macular SD-OCT volumes and microperimetry maps were obtained during the international, multicenter, randomized phase 2 trial of ciliary neurotrophic factor for type 2 MacTel on two visits within 5 days of one another. Software was developed to register SD-OCT to MAIA scanning laser ophthalmoscopy images and to overlay EZ defect areas on the microperimetry maps generated from microperimetry sensitivity values at specific points and from interpolated sensitivity values. A total of 134 eyes of 67 patients were investigated.
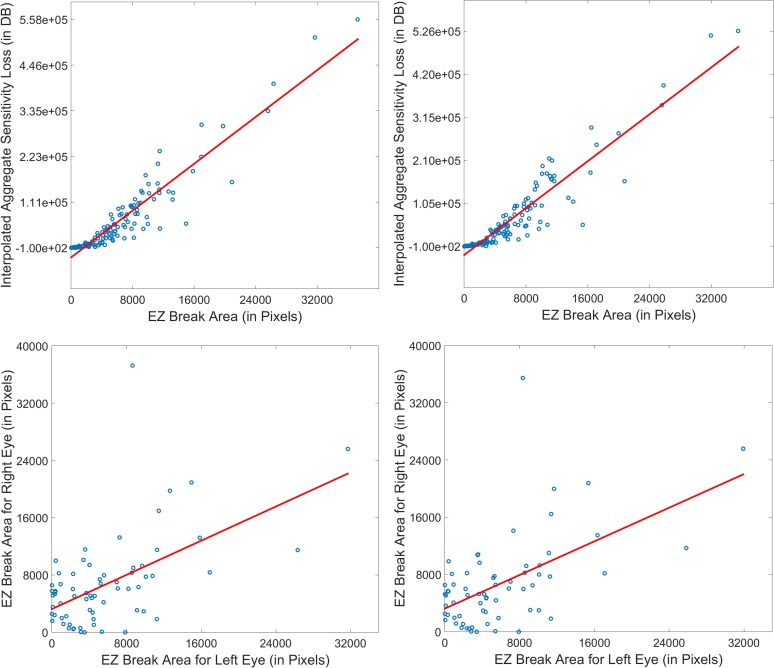
Results: The semiautomated registration algorithm was found to be accurate, both qualitatively by visual inspection of the nearly perfect overlap of the retinal vessels and quantitatively as assessed by interobserver reliability metrics performed in 98 eyes of 49 patients (intraclass correlation of aggregate retinal sensitivity loss >0.99). Aggregate retinal sensitivity loss within the EZ defect area was highly correlated with EZ defect area (Pearson correlation coefficient 0.93 and 0.92 at screening and baseline for noninterpolated maps; both were 0.94 for interpolated maps; P values <0.001).
Conclusions: With our software and image processing algorithms, there is nearly perfect correlation between retinal sensitivity on microperimetry and EZ defect area on SD-OCT. Our software allows determination of functional and structural changes with increasing disease severity and demonstrates that functional loss on microperimetry may be used as a surrogate marker of EZ loss on SD-OCT in type 2 MacTel.
Figures
Similar articles
-
Progression of vascular changes in macular telangiectasia type 2: comparison between SD-OCT and OCT angiography.Graefes Arch Clin Exp Ophthalmol. 2019 Jul;257(7):1381-1392. doi: 10.1007/s00417-019-04323-0. Epub 2019 May 16. Graefes Arch Clin Exp Ophthalmol. 2019. PMID: 31093765
-
Functional Relevance of Hyper-Reflectivity in Macular Telangiectasia Type 2.Invest Ophthalmol Vis Sci. 2021 Mar 1;62(3):6. doi: 10.1167/iovs.62.3.6. Invest Ophthalmol Vis Sci. 2021. PMID: 33661283 Free PMC article. Clinical Trial.
-
OCT Angiography and Ellipsoid Zone Mapping of Macular Telangiectasia Type 2 From the AVATAR Study.Invest Ophthalmol Vis Sci. 2017 Jul 1;58(9):3683-3689. doi: 10.1167/iovs.16-20976. Invest Ophthalmol Vis Sci. 2017. PMID: 28727884 Free PMC article.
-
Imaging endpoints for clinical trials in MacTel type 2.Eye (Lond). 2022 Feb;36(2):284-293. doi: 10.1038/s41433-021-01723-7. Epub 2021 Aug 13. Eye (Lond). 2022. PMID: 34389818 Free PMC article. Review.
-
Macular telangiectasia type 2.Prog Retin Eye Res. 2013 May;34:49-77. doi: 10.1016/j.preteyeres.2012.11.002. Epub 2012 Dec 3. Prog Retin Eye Res. 2013. PMID: 23219692 Free PMC article. Review.
Cited by
-
Serine and Lipid Metabolism in Macular Disease and Peripheral Neuropathy.N Engl J Med. 2019 Oct 10;381(15):1422-1433. doi: 10.1056/NEJMoa1815111. Epub 2019 Sep 11. N Engl J Med. 2019. PMID: 31509666 Free PMC article.
-
Beyond Performance Metrics: Automatic Deep Learning Retinal OCT Analysis Reproduces Clinical Trial Outcome.Ophthalmology. 2020 Jun;127(6):793-801. doi: 10.1016/j.ophtha.2019.12.015. Epub 2019 Dec 23. Ophthalmology. 2020. PMID: 32019699 Free PMC article. Clinical Trial.
-
The Natural History of Retinal Sensitivity Loss in Diabetic Macular Ischemia over One Year Evaluated by Microperimetry.J Clin Med. 2024 Apr 11;13(8):2219. doi: 10.3390/jcm13082219. J Clin Med. 2024. PMID: 38673492 Free PMC article.
-
VALIDATION OF A DEEP LEARNING-BASED ALGORITHM FOR SEGMENTATION OF THE ELLIPSOID ZONE ON OPTICAL COHERENCE TOMOGRAPHY IMAGES OF AN USH2A-RELATED RETINAL DEGENERATION CLINICAL TRIAL.Retina. 2022 Jul 1;42(7):1347-1355. doi: 10.1097/IAE.0000000000003448. Retina. 2022. PMID: 35174801 Free PMC article. Clinical Trial.
-
Progression of vascular changes in macular telangiectasia type 2: comparison between SD-OCT and OCT angiography.Graefes Arch Clin Exp Ophthalmol. 2019 Jul;257(7):1381-1392. doi: 10.1007/s00417-019-04323-0. Epub 2019 May 16. Graefes Arch Clin Exp Ophthalmol. 2019. PMID: 31093765
References
-
- Charbel Issa P, Heeren TF, Kupitz EH, Holz FG, Berendschot TT. . Very early disease manifestations of macular telangiectasia type 2. Retina. 2016; 36: 524– 534. - PubMed
-
- Ooto S, Hangai M, Takayama K,et al. . High-resolution photoreceptor imaging in idiopathic macular telangiectasia type 2 using adaptive optics scanning laser ophthalmoscopy. Invest Ophthalmol Vis Sci. 2011; 52: 5541– 5550. - PubMed
-
- Charbel Issa P, Helb HM, Rohrschneider K, Holz FG, Scholl HP. . Microperimetric assessment of patients with type 2 idiopathic macular telangiectasia. Invest Ophthalmol Vis Sci. 2007; 48: 3788– 3795. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
