

Delirium in Older Persons: Advances in Diagnosis and Treatment
- PMID: 28973626
- PMCID: PMC5717753
- DOI: 10.1001/jama.2017.12067
Delirium in Older Persons: Advances in Diagnosis and Treatment
Abstract
Importance: Delirium is defined as an acute disorder of attention and cognition. It is a common, serious, and often fatal condition among older patients. Although often underrecognized, delirium has serious adverse effects on the individual's function and quality of life, as well as broad societal effects with substantial health care costs.
Objective: To summarize the current state of the art in diagnosis and treatment of delirium and to highlight critical areas for future research to advance the field.
Evidence review: Search of Ovid MEDLINE, Embase, and the Cochrane Library for the past 6 years, from January 1, 2011, until March 16, 2017, using a combination of controlled vocabulary and keyword terms. Since delirium is more prevalent in older adults, the focus was on studies in elderly populations; studies based solely in the intensive care unit (ICU) and non-English-language articles were excluded.
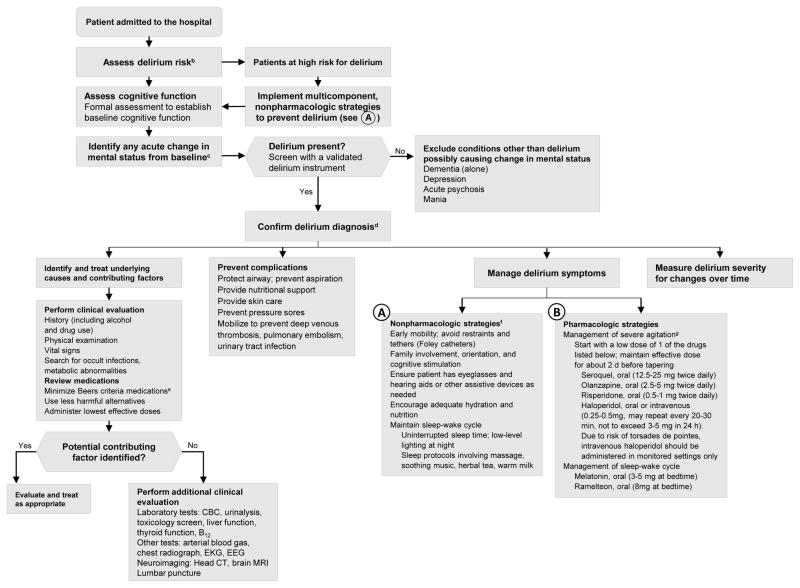
Findings: Of 127 articles included, 25 were clinical trials, 42 cohort studies, 5 systematic reviews and meta-analyses, and 55 were other categories. A total of 11 616 patients were represented in the treatment studies. Advances in diagnosis have included the development of brief screening tools with high sensitivity and specificity, such as the 3-Minute Diagnostic Assessment; 4 A's Test; and proxy-based measures such as the Family Confusion Assessment Method. Measures of severity, such as the Confusion Assessment Method-Severity Score, can aid in monitoring response to treatment, risk stratification, and assessing prognosis. Nonpharmacologic approaches focused on risk factors such as immobility, functional decline, visual or hearing impairment, dehydration, and sleep deprivation are effective for delirium prevention and also are recommended for delirium treatment. Current recommendations for pharmacologic treatment of delirium, based on recent reviews of the evidence, recommend reserving use of antipsychotics and other sedating medications for treatment of severe agitation that poses risk to patient or staff safety or threatens interruption of essential medical therapies.
Conclusions and relevance: Advances in diagnosis can improve recognition and risk stratification of delirium. Prevention of delirium using nonpharmacologic approaches is documented to be effective, while pharmacologic prevention and treatment of delirium remains controversial.
Figures
References
-
- Hustey F, Meldon S, Palmer R. Prevalence and documentation of impaired mental status in elderly emergency department patients. Acad Emerge Med. 2000;7(10):1166–1166. - PubMed
-
- Inouye SK, Foreman MD, Mion LC, Katz KH, Cooney LM., Jr Nurses’ recognition of delirium and its symptoms: comparison of nurse and researcher ratings. Arch Intern Med. 2001;161(20):2467–2473. - PubMed
-
- de la Cruz M, Fan J, Yennu S, et al. The frequency of missed delirium in patients referred to palliative care in comprehensive cancer center. Support Care Cancer. 2015;23(8):2427–2433. - PubMed
-
- American Psychiatric Association, editor. Diagnostic and Statistical Manual of Mental Disorders. 5. Washington, DC: American Psychiatric Society; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
