

Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis
- PMID: 28973656
- PMCID: PMC5838579
- DOI: 10.1001/jamaoncol.2017.3064
Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis
Abstract
Importance: If not promptly recognized, endocrine dysfunction can be life threatening. The incidence and risk of developing such adverse events (AEs) following the use of immune checkpoint inhibitor (ICI) regimens are unknown.
Objective: To compare the incidence and risk of endocrine AEs following treatment with US Food and Drug Administration-approved ICI regimens.
Data sources: A PubMed search through July 18, 2016, using the following keywords was performed: "ipilimumab," "MDX-010," "nivolumab," "BMS-963558," "pembrolizumab," "MK-3475," "atezolizumab," "MPDL3280A," and "phase."
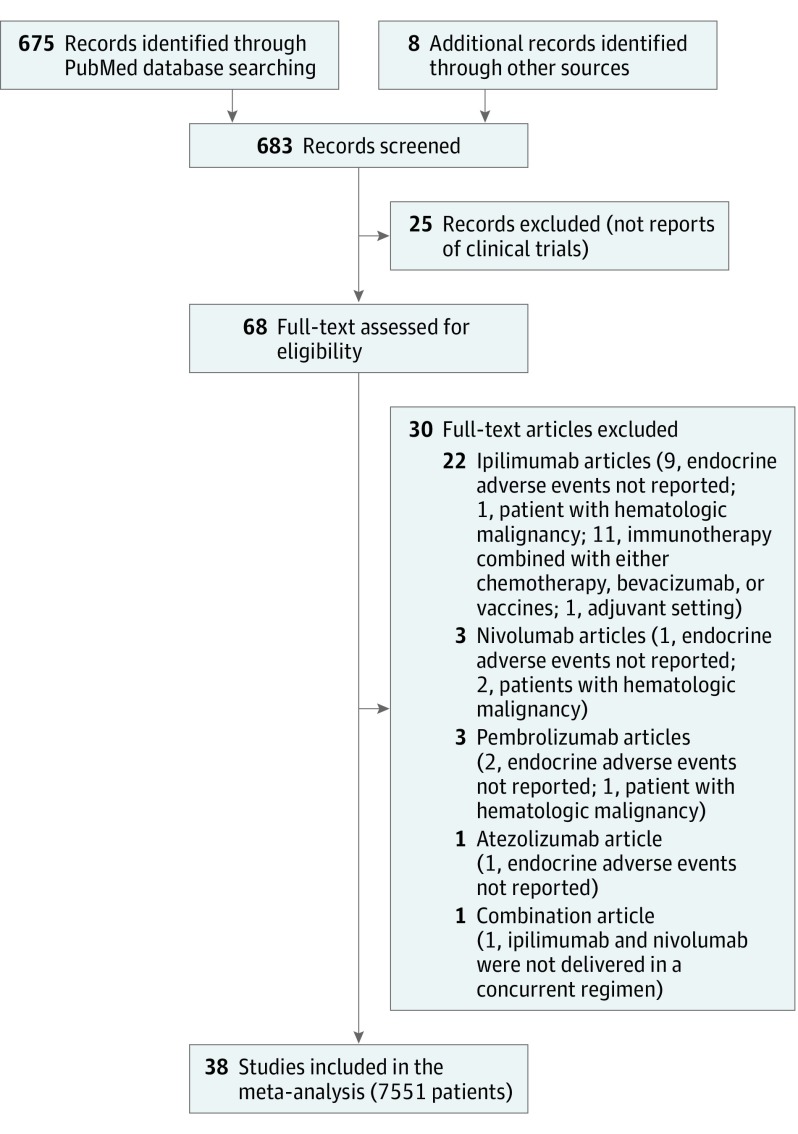
Study selection: Thirty-eight randomized clinical trials evaluating the usage of these ICIs for treatment of advanced solid tumors were identified, resulting in a total of 7551 patients who were eligible for a meta-analysis. Regimens were categorized by class into monotherapy with a PD-1 (programmed cell death protein 1) inhibitor, a CTLA-4 (cytotoxic T-lymphocyte-associated protein-4) inhibitor, or a PD-L1 (programmed cell death 1 ligand 1) inhibitor, and combination therapy with PD-1 plus CTLA-4 inhibitors.
Data extraction and synthesis: The data were extracted by 1 primary reviewer (R.B.-S.) and then independently reviewed by 2 secondary reviewers (W.T.B. and A.C.G.-C.) following Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. Inferences on the incidence of AEs were made using log-odds random effects models.
Main outcomes and measures: Incidence of all-grade hypothyroidism, hyperthyroidism, hypophysitis, primary adrenal insufficiency, and insulin-deficient diabetes.
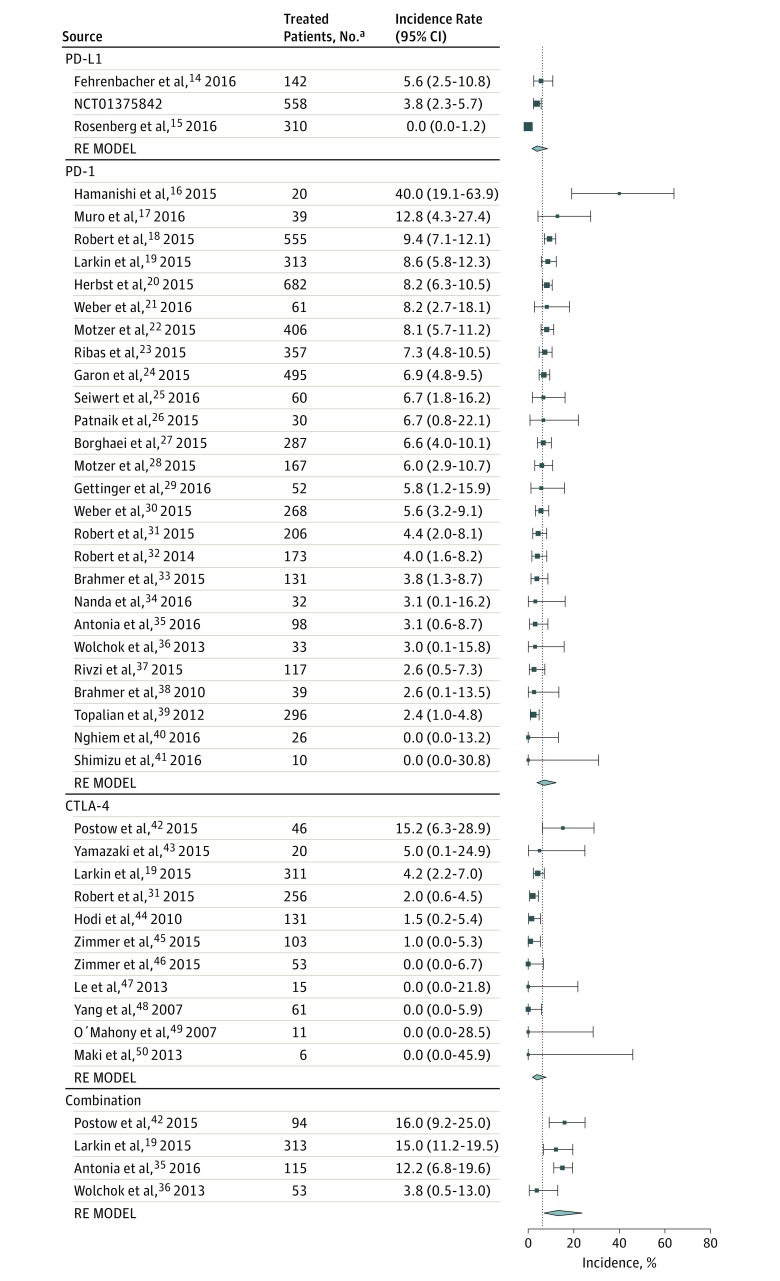
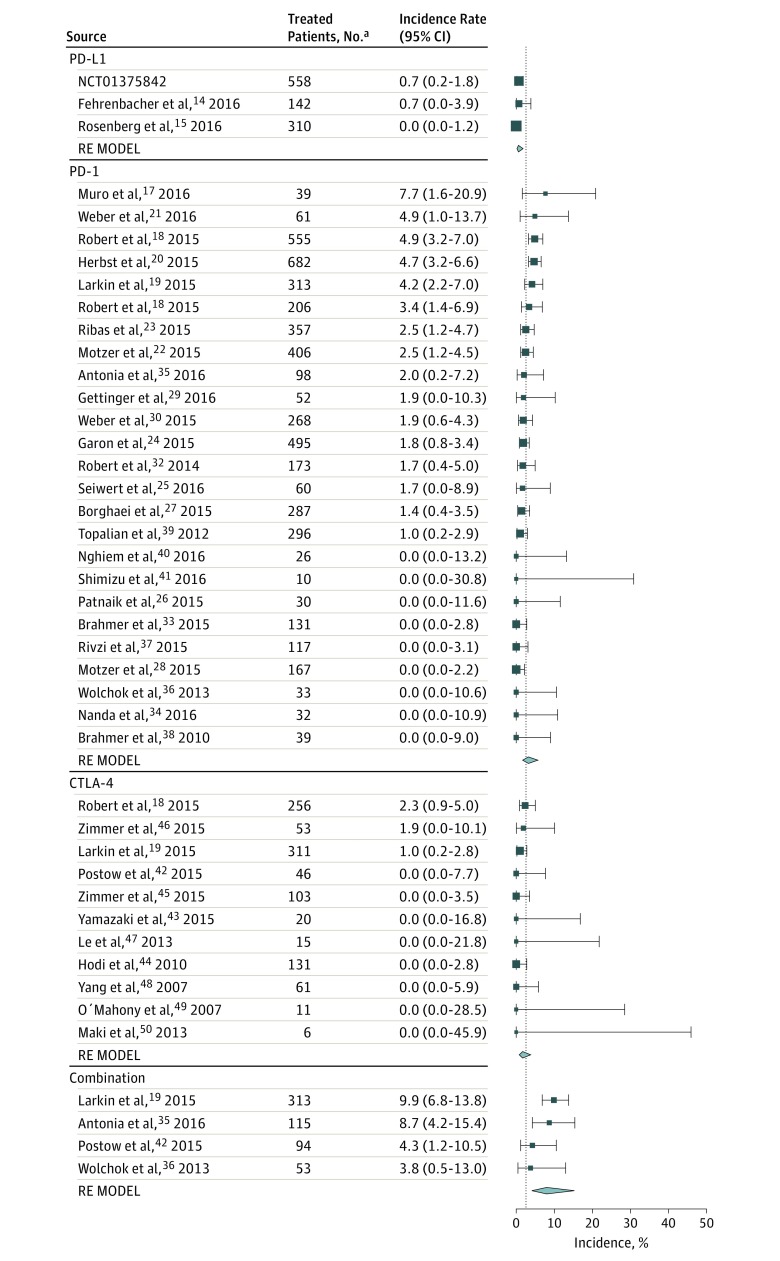
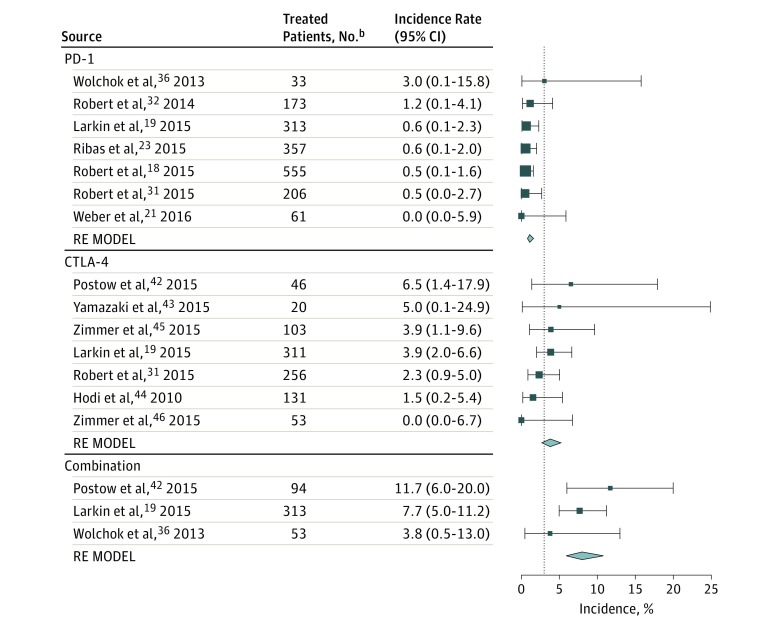
Results: Overall, 38 randomized clinical trials comprising 7551 patients were included in this systematic review and meta-analysis. The incidence of both hypothyroidism and hyperthyroidism was highest in patients receiving combination therapy. Patients on the combination regimen were significantly more likely to experience hypothyroidism (odds ratio [OR], 3.81; 95% CI, 2.10-6.91, P < .001) and hyperthyroidism (OR, 4.27; 95% CI, 2.05-8.90; P = .001) than patients on ipilimumab. Compared with patients on ipilimumab, those on PD-1 inhibitors had a higher risk of developing hypothyroidism (OR, 1.89; 95% CI, 1.17-3.05; P = .03). The risk of hyperthyroidism, but not hypothyroidism, was significantly greater with PD-1 than with PD-L1 inhibitors (OR, 5.36; 95% CI, 2.04-14.08; P = .002). While patients who received PD-1 inhibitors were significantly less likely to experience hypophysitis than those receiving ipilimumab (OR, 0.29; 95% CI, 0.18-0.49; P < .001), those who received combination therapy were significantly more likely to develop it (OR, 2.2; 95% CI, 1.39-3.60; P = .001). For primary adrenal insufficiency and insulin-deficient diabetes no statistical inferences were made due to the smaller number of events.
Conclusions and relevance: Our study provides more precise data on the incidence of endocrine dysfunctions among patients receiving ICI regimens. Patients on combination therapy are at increased risk of thyroid dysfunction and hypophysitis.
Conflict of interest statement
Figures
Comment in
-
Database Selection and Heterogeneity-More Details, More Credibility.JAMA Oncol. 2018 Sep 1;4(9):1295. doi: 10.1001/jamaoncol.2018.1209. JAMA Oncol. 2018. PMID: 29955774 No abstract available.
-
Database Selection and Heterogeneity-More Details, More Credibility-Reply.JAMA Oncol. 2018 Sep 1;4(9):1295-1296. doi: 10.1001/jamaoncol.2018.1231. JAMA Oncol. 2018. PMID: 29955794 No abstract available.
References
-
- Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271(5256):1734-1736. - PubMed
-
- Wolchok JD. PD-1 Blockers. Cell. 2015;162(5):937. - PubMed
-
- Waterhouse P, Penninger JM, Timms E, et al. Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science. 1995;270(5238):985-988. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
