

Mobile Phone-Based Measures of Activity, Step Count, and Gait Speed: Results From a Study of Older Ambulatory Adults in a Naturalistic Setting
- PMID: 28974482
- PMCID: PMC5645644
- DOI: 10.2196/mhealth.5090
Mobile Phone-Based Measures of Activity, Step Count, and Gait Speed: Results From a Study of Older Ambulatory Adults in a Naturalistic Setting
Abstract
Background: Cellular mobile telephone technology shows much promise for delivering and evaluating healthcare interventions in cost-effective manners with minimal barriers to access. There is little data demonstrating that these devices can accurately measure clinically important aspects of individual functional status in naturalistic environments outside of the laboratory.
Objective: The objective of this study was to demonstrate that data derived from ubiquitous mobile phone technology, using algorithms developed and previously validated by our lab in a controlled setting, can be employed to continuously and noninvasively measure aspects of participant (subject) health status including step counts, gait speed, and activity level, in a naturalistic community setting. A second objective was to compare our mobile phone-based data against current standard survey-based gait instruments and clinical physical performance measures in order to determine whether they measured similar or independent constructs.
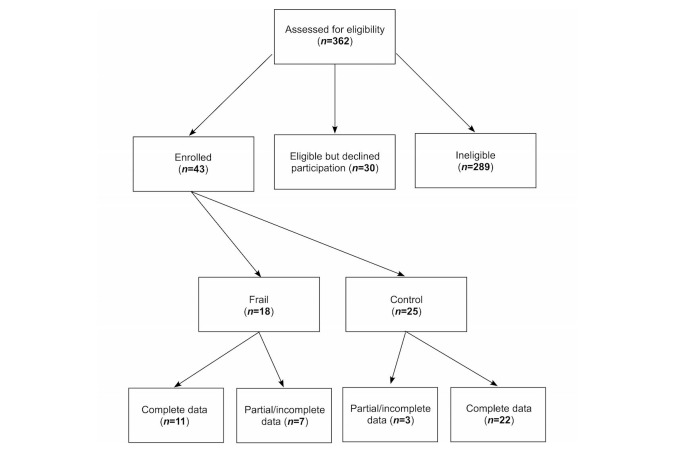
Methods: A total of 43 ambulatory, independently dwelling older adults were recruited from Nebraska Medicine, including 25 (58%, 25/43) healthy control individuals from our Engage Wellness Center and 18 (42%, 18/43) functionally impaired, cognitively intact individuals (who met at least 3 of 5 criteria for frailty) from our ambulatory Geriatrics Clinic. The following previously-validated surveys were obtained on study day 1: (1) Late Life Function and Disability Instrument (LLFDI); (2) Survey of Activities and Fear of Falling in the Elderly (SAFFE); (3) Patient Reported Outcomes Measurement Information System (PROMIS), short form version 1.0 Physical Function 10a (PROMIS-PF); and (4) PROMIS Global Health, short form version 1.1 (PROMIS-GH). In addition, clinical physical performance measurements of frailty (10 foot Get up and Go, 4 Meter walk, and Figure-of-8 Walk [F8W]) were also obtained. These metrics were compared to our mobile phone-based metrics collected from the participants in the community over a 24-hour period occurring within 1 week of the initial assessment.
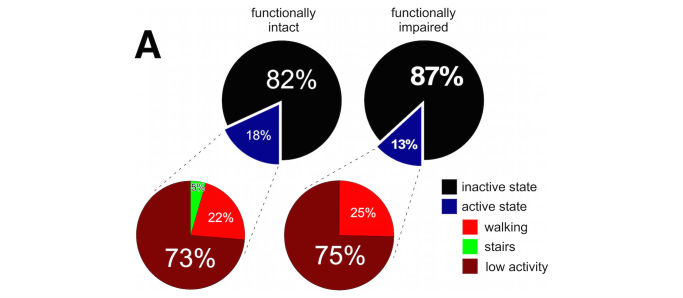
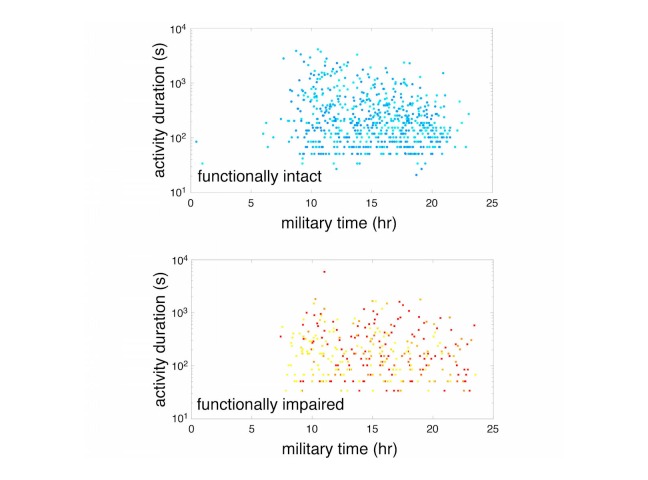
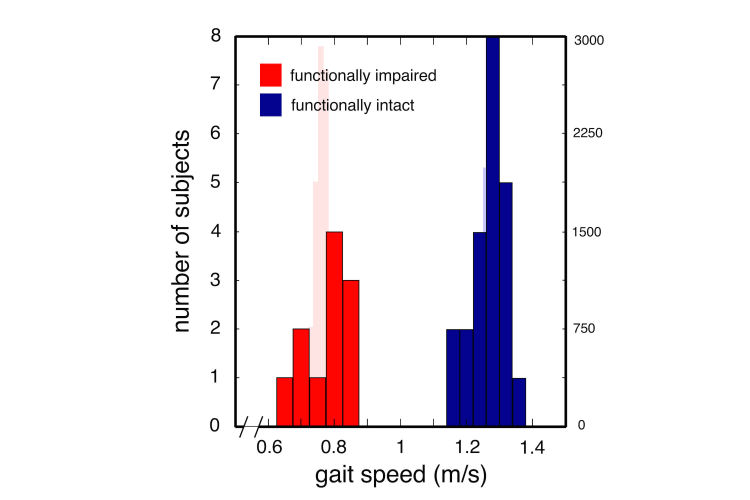
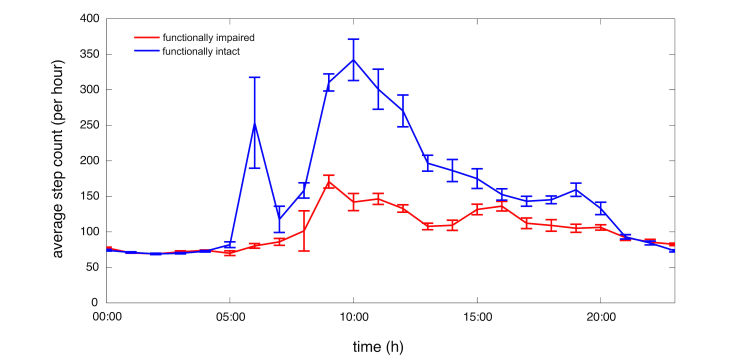
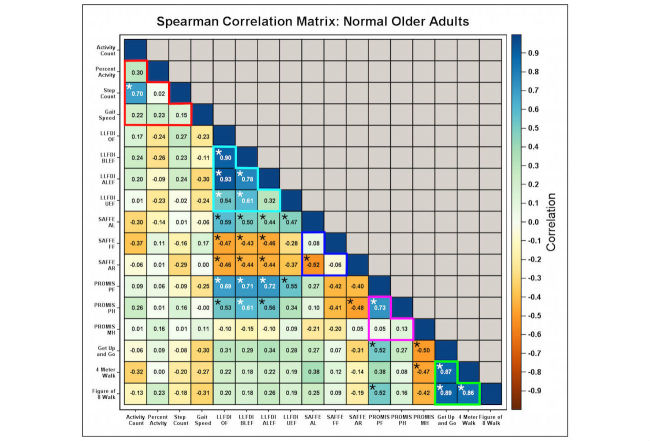
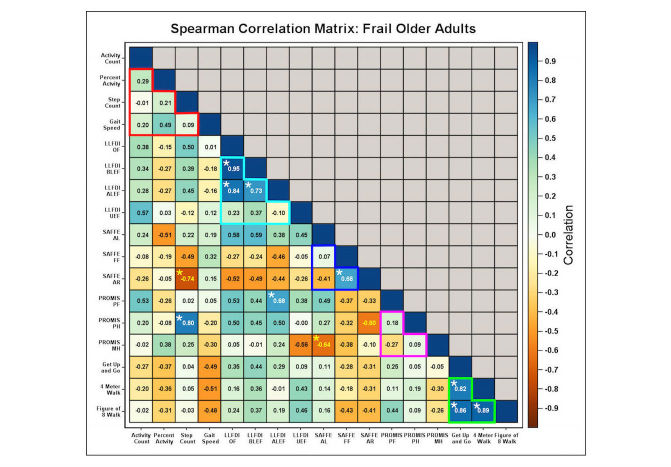
Results: We identified statistically significant differences between functionally intact and frail participants in mobile phone-derived measures of percent activity (P=.002, t test), active versus inactive status (P=.02, t test), average step counts (P<.001, repeated measures analysis of variance [ANOVA]) and gait speed (P<.001, t test). In functionally intact individuals, the above mobile phone metrics assessed aspects of functional status independent (Bland-Altman and correlation analysis) of both survey- and/or performance battery-based functional measures. In contrast, in frail individuals, the above mobile phone metrics correlated with submeasures of both SAFFE and PROMIS-GH.
Conclusions: Continuous mobile phone-based measures of participant community activity and mobility strongly differentiate between persons with intact functional status and persons with a frailty phenotype. These measures assess dimensions of functional status independent of those measured using current validated questionnaires and physical performance assessments to identify functional compromise. Mobile phone-based gait measures may provide a more readily accessible and less-time consuming measure of gait, while further providing clinicians with longitudinal gait measures that are currently difficult to obtain.
Keywords: LLFDI; PROMIS Global; PROMIS short; SAFFE; behavioral classification; frailty phenotype; functional status; gait speed; mobile phone; mobility; mobility measures; normal aging; step count.
©Cassia Rye Hanton, Yong-Jun Kwon, Thawda Aung, Jackie Whittington, Robin R High, Evan H Goulding, A Katrin Schenk, Stephen J Bonasera. Originally published in JMIR Mhealth and Uhealth (http://mhealth.jmir.org), 03.10.2017.
Conflict of interest statement
Conflicts of Interest: SJB, AKS, and EHG have received a patent regarding aspects of this technological approach (US Patent 9,106,718 B2; Lifespace data collection from discrete areas).
Figures
References
-
- Pahor M, Guralnik JM, Ambrosius WT, Blair S, Bonds DE, Church TS, Espeland MA, Fielding RA, Gill TM, Groessl EJ, King AC, Kritchevsky SB, Manini TM, McDermott MM, Miller ME, Newman AB, Rejeski WJ, Sink KM, Williamson JD, LIFE study investigators Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA. 2014 Jun 18;311(23):2387–96. doi: 10.1001/jama.2014.5616. http://europepmc.org/abstract/MED/24866862 - DOI - PMC - PubMed
-
- Dodge HH, Mattek NC, Austin D, Hayes TL, Kaye JA. In-home walking speeds and variability trajectories associated with mild cognitive impairment. Neurology. 2012 Jun 12;78(24):1946–52. doi: 10.1212/WNL.0b013e318259e1de. http://europepmc.org/abstract/MED/22689734 - DOI - PMC - PubMed
-
- Abellan van Kan G, Rolland Y, Andrieu S, Bauer J, Beauchet O, Bonnefoy M, Cesari M, Donini LM, Gillette GS, Inzitari M, Nourhashemi F, Onder G, Ritz P, Salva A, Visser M, Vellas B. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009 Dec;13(10):881–9. - PubMed
-
- Hardy SE, Kang Y, Studenski SA, Degenholtz HB. Ability to walk 1/4 mile predicts subsequent disability, mortality, and health care costs. J Gen Intern Med. 2011 Feb;26(2):130–5. doi: 10.1007/s11606-010-1543-2. http://europepmc.org/abstract/MED/20972641 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
