

Delayed Repolarization Underlies Ventricular Arrhythmias in Rats With Heart Failure and Preserved Ejection Fraction
- PMID: 28974519
- PMCID: PMC5698112
- DOI: 10.1161/CIRCULATIONAHA.117.028202
Delayed Repolarization Underlies Ventricular Arrhythmias in Rats With Heart Failure and Preserved Ejection Fraction
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) represents approximately half of heart failure, and its incidence continues to increase. The leading cause of mortality in HFpEF is sudden death, but little is known about the underlying mechanisms.
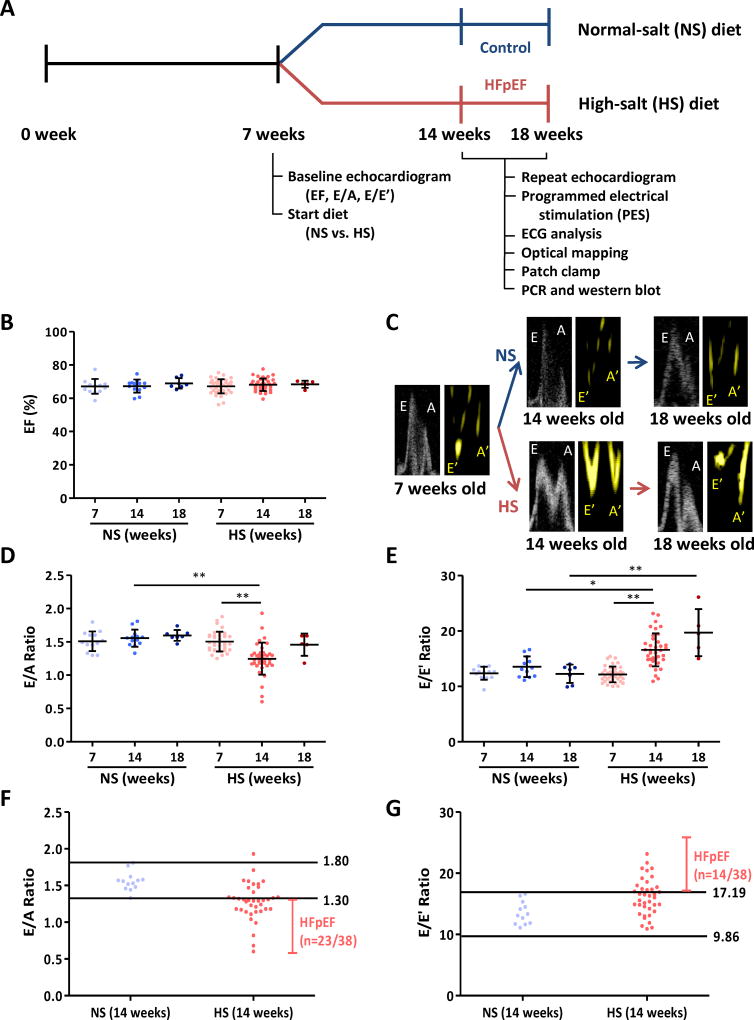
Methods: Dahl salt-sensitive rats were fed a high-salt diet (8% NaCl) from 7 weeks of age to induce HFpEF (n=38). Rats fed a normal-salt diet (0.3% NaCl) served as controls (n=13). Echocardiograms were performed to assess systolic and diastolic function from 14 weeks of age. HFpEF-verified and control rats underwent programmed electrical stimulation. Corrected QT interval was measured by surface ECG. The mechanisms of ventricular arrhythmias (VA) were probed by optical mapping, whole-cell patch clamp to measure action potential duration and ionic currents, and quantitative polymerase chain reaction and Western blotting to investigate changes in ion channel expression.
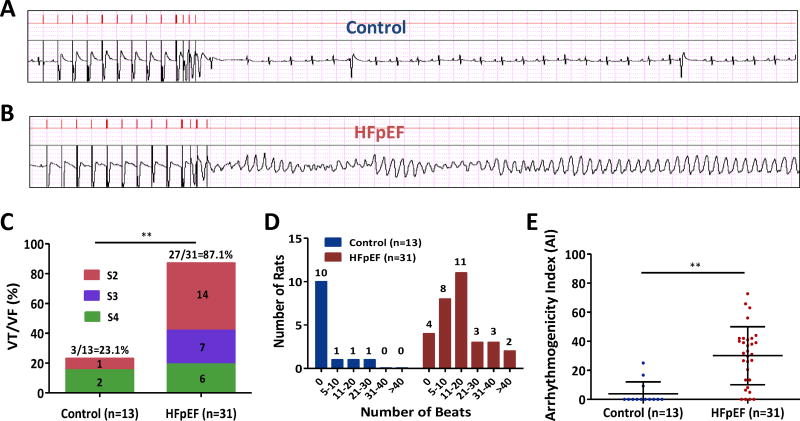
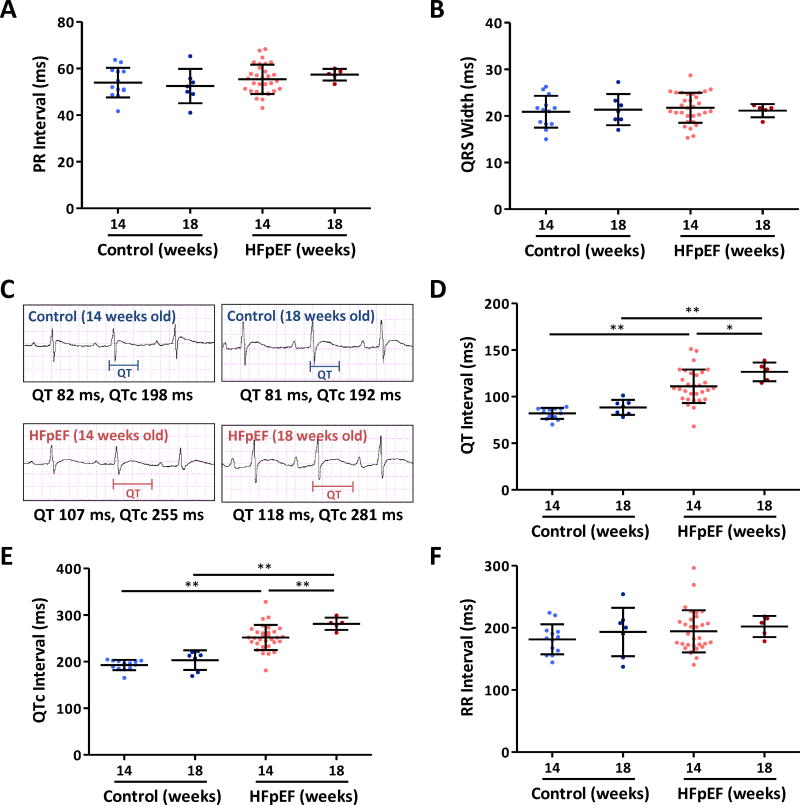
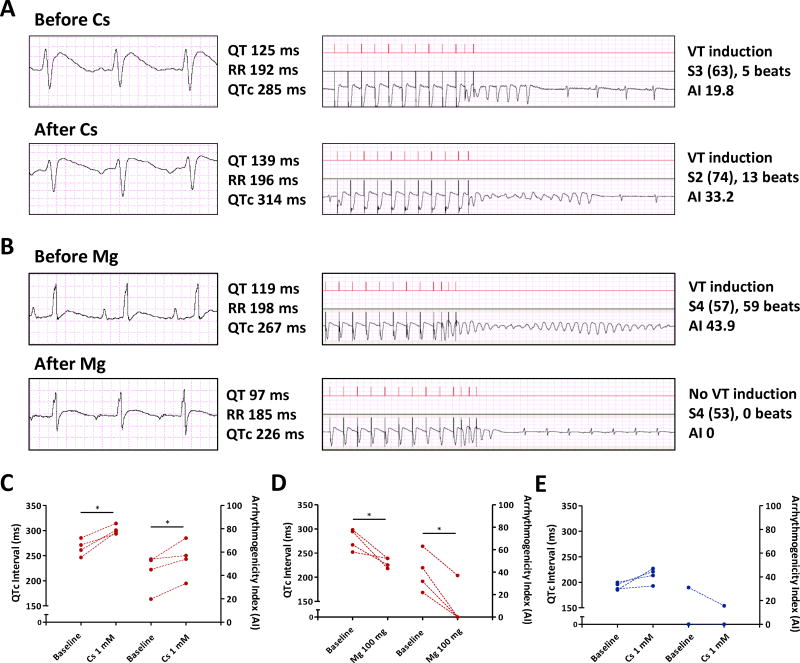
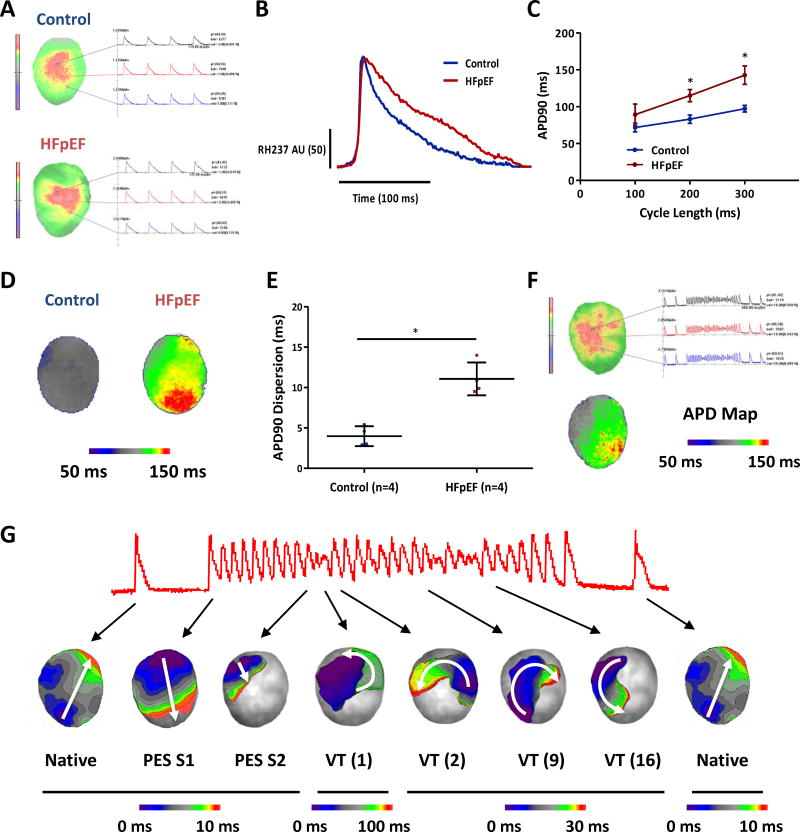
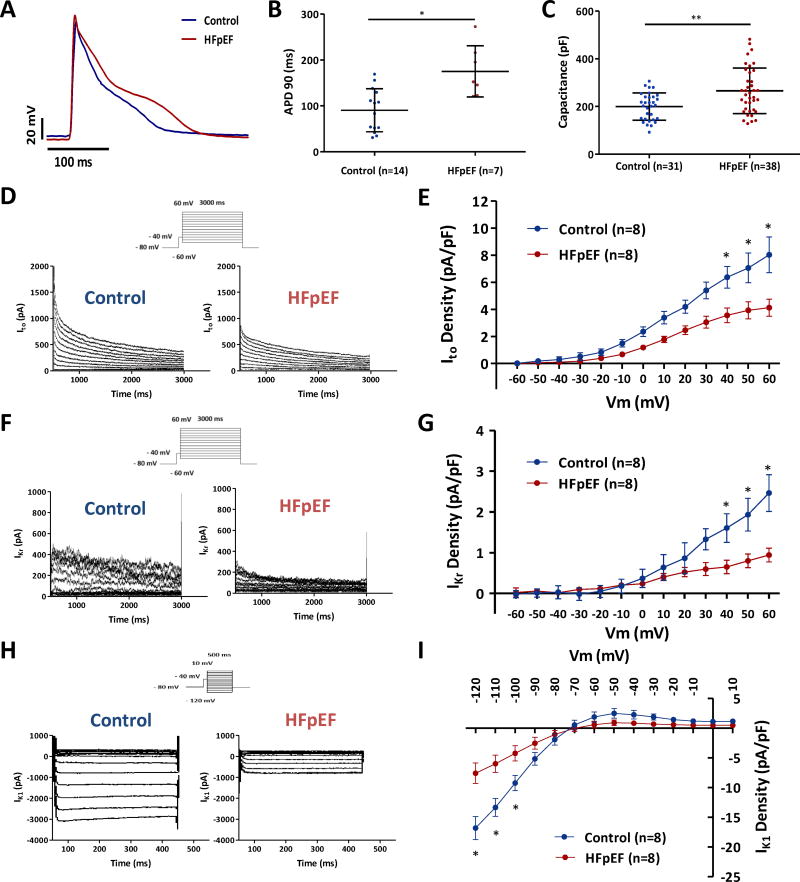
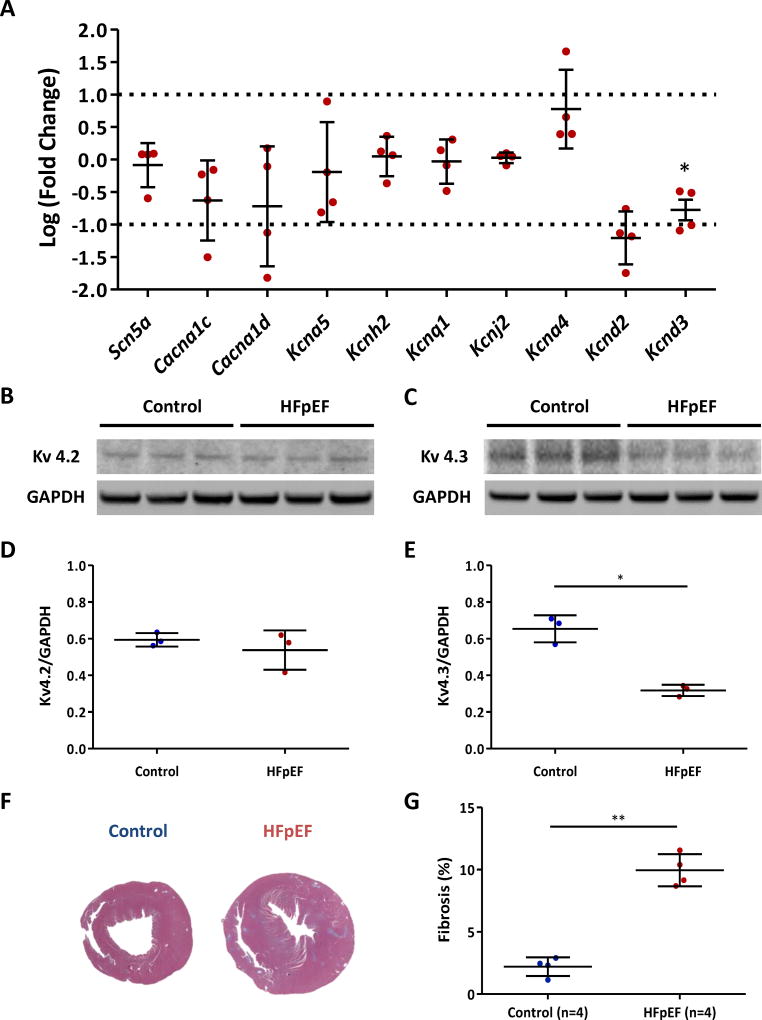
Results: After 7 weeks of a high-salt diet, 31 of 38 rats showed diastolic dysfunction and preserved ejection fraction along with signs of heart failure and hence were diagnosed with HFpEF. Programmed electric stimulation demonstrated increased susceptibility to VA in HFpEF rats (P<0.001 versus controls). The arrhythmogenicity index was increased (P<0.001) and the corrected QT interval on ECG was prolonged (P<0.001) in HFpEF rats. Optical mapping of HFpEF hearts demonstrated prolonged action potentials (P<0.05) and multiple reentry circuits during induced VA. Single-cell recordings of cardiomyocytes isolated from HFpEF rats confirmed a delay of repolarization (P=0.001) and revealed downregulation of transient outward potassium current (Ito; P<0.05). The rapid components of the delayed rectifier potassium current (IKr) and the inward rectifier potassium current (IK1) were also downregulated (P<0.05), but the current densities were much lower than for Ito. In accordance with the reduction of Ito, both Kcnd3 transcript and Kv4.3 protein levels were decreased in HFpEF rat hearts.
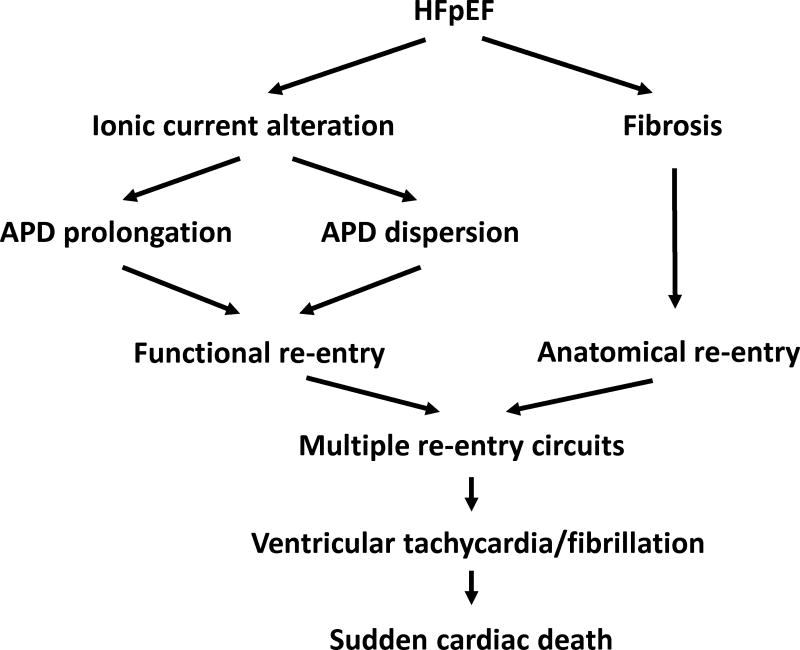
Conclusions: Susceptibility to VA was markedly increased in rats with HFpEF. Underlying abnormalities include QT prolongation, delayed repolarization from downregulation of potassium currents, and multiple reentry circuits during VA. Our findings are consistent with the hypothesis that potassium current downregulation leads to abnormal repolarization in HFpEF, which in turn predisposes to VA and sudden cardiac death.
Keywords: action potentials; arrhythmias, cardiac; death, sudden; fibrosis; heart failure; patch-clamp techniques; potassium channels.
© 2017 American Heart Association, Inc.
Figures
References
-
- Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: Final Data for 2014. Natl Vital Stat Rep. 2016;65:1–122. - PubMed
-
- Writing Committee M; Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL American College of Cardiology Foundation/American Heart Association Task Force on Practice G. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128:e240–327. - PubMed
-
- Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348:2007–2018. - PubMed
-
- Braunwald E. Heart failure. JACC Heart Fail. 2013;1:1–20. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
