

Randomized controlled trial of uncut Roux-en-Y vs Billroth II reconstruction after distal gastrectomy for gastric cancer: Which technique is better for avoiding biliary reflux and gastritis?
- PMID: 28974902
- PMCID: PMC5603502
- DOI: 10.3748/wjg.v23.i34.6350
Randomized controlled trial of uncut Roux-en-Y vs Billroth II reconstruction after distal gastrectomy for gastric cancer: Which technique is better for avoiding biliary reflux and gastritis?
Abstract
Aim: To identify which technique is better for avoiding biliary reflux and gastritis between uncut Roux-en-Y and Billroth II reconstruction.
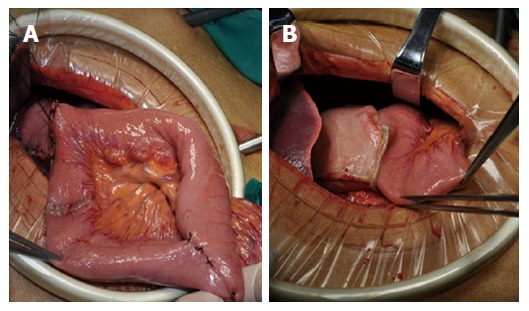
Methods: A total of 158 patients who underwent laparoscopy-assisted distal gastrectomy for gastric cancer at the First Hospital of Jilin University (Changchun, China) between February 2015 and February 2016 were randomized into two groups: uncut Roux-en-Y (group U) and Billroth II group (group B). Postoperative complications and relevant clinical data were compared between the two groups.
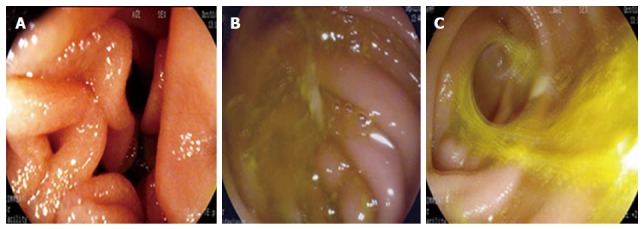
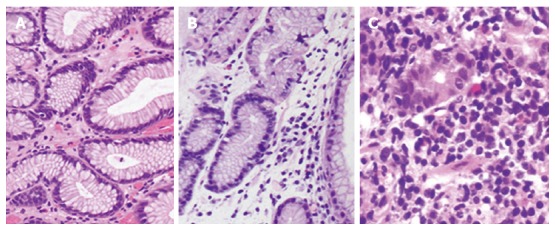
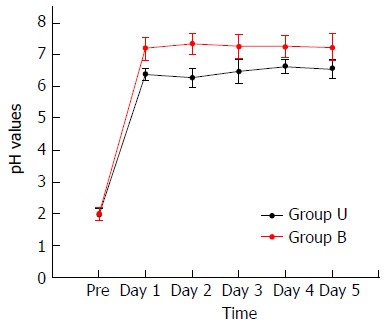
Results: According to the randomization table, each group included 79 patients. There was no significant difference in postoperative complications between groups U and B (7.6% vs 10.1%, P = 0.576). During the postoperative period, group U stomach pH values were lower than 7 and group B pH values were higher than 7. After 1 year of follow-up, group B presented a higher incidence of biliary reflux and alkaline gastritis. However, histopathology did not show a significant difference in gastritis diagnosis (P = 0.278), and the amount of residual food and gain of weight between the groups were also not significantly different. At 3 mo there was no evidence of partial recanalization of uncut staple line, but at 1 year the incidence was 13%.
Conclusion: Compared with Billroth II reconstruction, uncut Roux-en-Y reconstruction is secure and feasible, and can effectively reduce the incidence of alkaline reflux, residual gastritis, and heartburn. Despite the incidence of recanalization, uncut Roux-en-Y should be widely applied.
Keywords: Alkaline gastritis; Bile reflux; Billroth II; Gastric cancer; Uncut Roux-en-Y.
Conflict of interest statement
Conflict-of-interest statement: All authors declare no conflict of interest.
Figures
References
-
- Lee MS, Ahn SH, Lee JH, Park DJ, Lee HJ, Kim HH, Yang HK, Kim N, Lee WW. What is the best reconstruction method after distal gastrectomy for gastric cancer? Surg Endosc. 2012;26:1539–1547. - PubMed
-
- Tran TB, Worhunsky DJ, Squires MH, Jin LX, Spolverato G, Votanopoulos KI, Cho CS, Weber SM, Schmidt C, Levine EA, et al. To Roux or not to Roux: a comparison between Roux-en-Y and Billroth II reconstruction following partial gastrectomy for gastric cancer. Gastric Cancer. 2016;19:994–1001. - PubMed
-
- Hatta W, Gotoda T, Oyama T, Kawata N, Takahashi A, Yoshifuku Y, Hoteya S, Nakamura K, Hirano M, Esaki M, et al. Is radical surgery necessary in all patients who do not meet the curative criteria for endoscopic submucosal dissection in early gastric cancer? A multi-center retrospective study in Japan. J Gastroenterol. 2017;52:175–184. - PubMed
-
- Uyama I, Sakurai Y, Komori Y, Nakamura Y, Syoji M, Tonomura S, Yoshida I, Masui T, Inaba K, Ochiai M. Laparoscopy-assisted uncut Roux-en-Y operation after distal gastrectomy for gastric cancer. Gastric Cancer. 2005;8:253–257. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
