Two-phase laparoendoscopic single-site cervical ligament-sparing hysterectomy: An initial experience
- PMID: 28974911
- PMCID: PMC5615997
- DOI: 10.4103/tcmj.tcmj_61_17
Two-phase laparoendoscopic single-site cervical ligament-sparing hysterectomy: An initial experience
Abstract
Objective: To report our initial experience with and the short-term outcomes of two-phase laparoendoscopic single-site cervical ligament-sparing hysterectomy (LESS-CLSH).
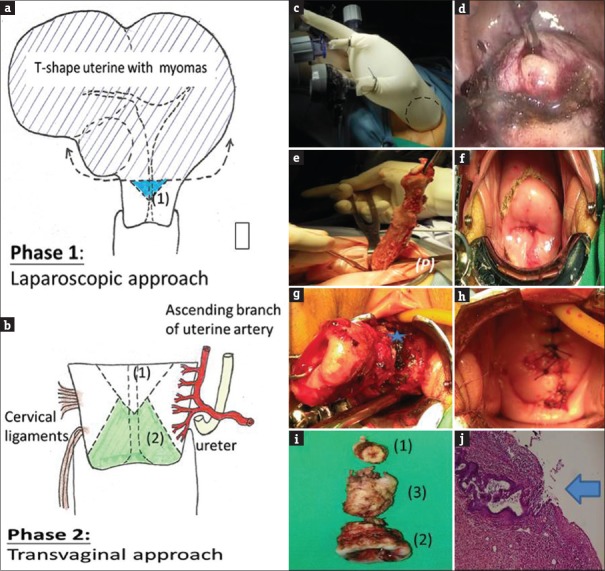
Materials and methods: A retrospective case study included 40 women who underwent LESS-CLSH from January 2014 to December 2016 at Buddhist Tzu Chi General Hospital. Uterine specimens were extracted through contained manual morcellation with a tissue pouch. The first phase was LESS supracervical hysterectomy and conization of the internal orifice of the cervix. The second phase was transvaginal cervical conization and cylinderization. Women with a uterus diameter of >12 cm, a broad ligament myoma, or severe pelvic adhesion were categorized into a difficult group, and others were categorized into a nondifficult group.
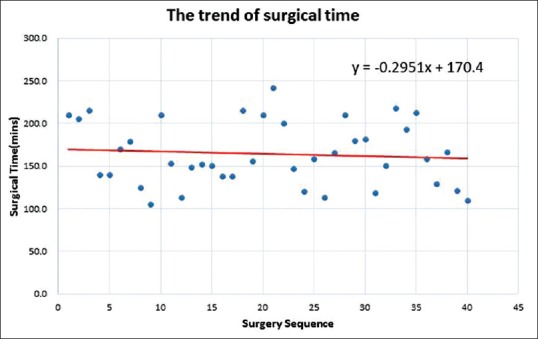
Results: The difficult group required more time and had more blood loss than the nondifficult group. The mean surgical time was 187.2 ± 33.9 and 139.1 ± 20.7 min, and the mean blood loss was 533.3 ± 333.3 and 225.3 ± 168.2 mL in the difficult and nondifficult groups, respectively. The overall visual analog scale (VAS) pain scores at 0-4, 24, and 48 h after surgery were 7.1 ± 1.9, 4.2 ± 1.6, and 2.3 ± 1.5, respectively; no difference in the VAS pain scores, pain relief score, and hospitalization duration was observed between the two groups. Minor surgical complications or adverse events on follow-up were noted. Three months after surgery, the diameter and thickness of the cervix were decreased by approximately 0.5 and 1.0 cm, respectively.
Conclusion: LESS-CLSH is a minimally invasive, safe, and feasible approach, even for difficult laparoscopic hysterectomy. Contained manual morcellation enables more controlled specimen removal than morcellation only.
Keywords: Cervical ligament sparing; Hysterectomy; Laparoendoscopic single site; Single port.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Robotic laparoendoscopic single-site compared with robotic multi-port sacrocolpopexy for apical compartment prolapse.Am J Obstet Gynecol. 2020 Apr;222(4):358.e1-358.e11. doi: 10.1016/j.ajog.2019.09.048. Epub 2019 Oct 4. Am J Obstet Gynecol. 2020. PMID: 31589864 Clinical Trial.
-
Laparoscopic Uterine Artery Occlusion Combined with Uterine-sparing Pelvic Plexus Block and Partial Adenomyomectomy for Adenomyosis: A Video Case Report.J Minim Invasive Gynecol. 2021 Oct;28(10):1681-1684. doi: 10.1016/j.jmig.2021.05.015. Epub 2021 May 26. J Minim Invasive Gynecol. 2021. PMID: 34051355
-
Two-phase laparoendoscopic single-site cervical ligament-sparing hysterectomy: A novel approach in difficult laparoscopic hysterectomy.Taiwan J Obstet Gynecol. 2016 Jun;55(3):423-6. doi: 10.1016/j.tjog.2016.04.019. Taiwan J Obstet Gynecol. 2016. PMID: 27343328
-
Meta-analysis of Laparoendoscopic Single-site and Vaginal Natural Orifice Transluminal Endoscopic Hysterectomy Compared with Multiport Hysterectomy: Real Benefits or Diminishing Returns?J Minim Invasive Gynecol. 2021 Mar;28(3):698-709.e1. doi: 10.1016/j.jmig.2020.11.029. Epub 2020 Dec 17. J Minim Invasive Gynecol. 2021. PMID: 33346073
-
Adenomyoma recurrence 7 years after laparoscopic supracervical hysterectomy: A case report and literature review.Medicine (Baltimore). 2023 Nov 17;102(46):e36089. doi: 10.1097/MD.0000000000036089. Medicine (Baltimore). 2023. PMID: 37986313 Free PMC article. Review.
References
-
- Chene G, Tardieu AS, Savary D, Krief M, Boda C, Anton-Bousquet MC, et al. Anatomical and functional results of McCall culdoplasty in the prevention of enteroceles and vaginal vault prolapse after vaginal hysterectomy. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:1007–11. - PubMed
-
- DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992;166:1717–24. - PubMed
-
- Valaitis SR, Stanton SL. Sacrocolpopexy: A retrospective study of a clinician's experience. Br J Obstet Gynaecol. 1994;101:518–22. - PubMed
-
- Altman D, Falconer C, Cnattingius S, Granath F. Pelvic organ prolapse surgery following hysterectomy on benign indications. Am J Obstet Gynecol. 2008;198:572.e1–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources