

Interpretability of Cancer Clinical Trial Results Using Restricted Mean Survival Time as an Alternative to the Hazard Ratio
- PMID: 28975263
- PMCID: PMC5824272
- DOI: 10.1001/jamaoncol.2017.2797
Interpretability of Cancer Clinical Trial Results Using Restricted Mean Survival Time as an Alternative to the Hazard Ratio
Abstract
Importance: In a comparative clinical study with progression-free survival (PFS) or overall survival (OS) as the end point, the hazard ratio (HR) is routinely used to design the study and to estimate the treatment effect at the end of the study. The clinical interpretation of the HR may not be straightforward, especially when the underlying model assumption is not valid. A robust procedure for study design and analysis that enables clinically meaningful interpretation of trial results is warranted.
Objective: To discuss issues of conventional trial design and analysis and to present alternatives to the HR using a recent immunotherapy study as an illustrative example.
Design, setting, and participants: By comparing 2 groups in a survival analysis, we discuss issues of using the HR and present the restricted mean survival time (RMST) as a summary measure of patients’ survival profile over time. We show how to use the difference or ratio in RMST between 2 groups as an alternative for designing and analyzing a clinical study with an immunotherapy study as an illustrative example.
Main outcomes and measures: Overall survival or PFS. Group contrast measures included HR, RMST difference or ratio, and the event rate difference.
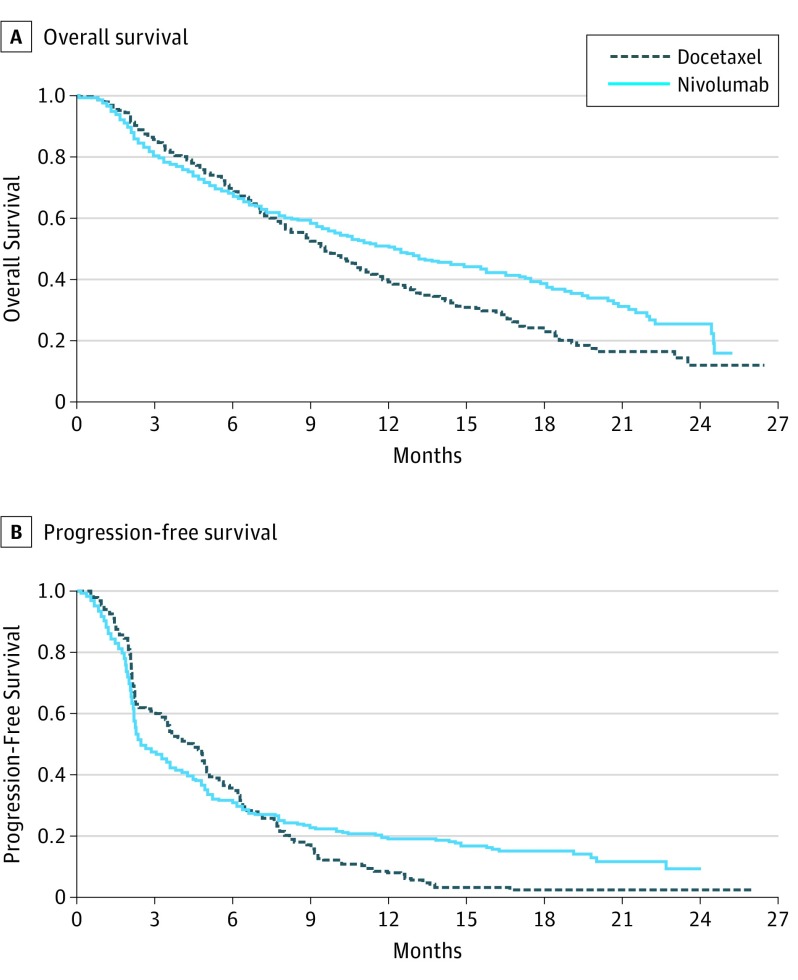
Results: For the illustrative example, the HR procedure indicates that nivolumab significantly prolonged patient OS and was numerically better than docetaxel for PFS. However, the median PFS time of docetaxel was significantly better than that of nivolumab. Therefore, it may be difficult to use median OS and/or PFS to interpret of the HR value clinically. On the other hand, using RMST difference, nivolumab was significantly better than docetaxel for both OS and PFS. We also provide details regarding design of a future study with RMST-based measures.
Conclusions and relevance: The design and analysis of a conventional cancer clinical trial can be improved by adopting a robust statistical procedure that enables clinically meaningful interpretations of the treatment effect. The RMST-based quantitative method may be used as a primary tool for future cancer trials or to help us to better understand the clinical interpretation of the HR even when its model assumption is plausible.
Conflict of interest statement
Figures

References
-
- Péron J, Roy P, Ozenne B, Roche L, Buyse M. The net chance of a longer survival as a patient-oriented measure of treatment benefit in randomized clinical trials. JAMA Oncol. 2016;2(7):901-905. - PubMed
-
- Chappell R, Zhu X. Describing differences in survival curves. JAMA Oncol. 2016;2(7):906-907. - PubMed
-
- Trinquart L, Jacot J, Conner SC, Porcher R. Comparison of treatment effects measured by the hazard ratio and by the ratio of restricted mean survival times in oncology randomized controlled trials. J Clin Oncol. 2016;34(15):1813-1819. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
