

Effect of a Community Health Worker-Led Multicomponent Intervention on Blood Pressure Control in Low-Income Patients in Argentina: A Randomized Clinical Trial
- PMID: 28975305
- PMCID: PMC5761321
- DOI: 10.1001/jama.2017.11358
Effect of a Community Health Worker-Led Multicomponent Intervention on Blood Pressure Control in Low-Income Patients in Argentina: A Randomized Clinical Trial
Abstract
Importance: Despite extensive knowledge of hypertension treatment, the prevalence of uncontrolled hypertension is high and increasing in low- and middle-income countries.
Objective: To test whether a community health worker-led multicomponent intervention would improve blood pressure (BP) control among low-income patients with hypertension.
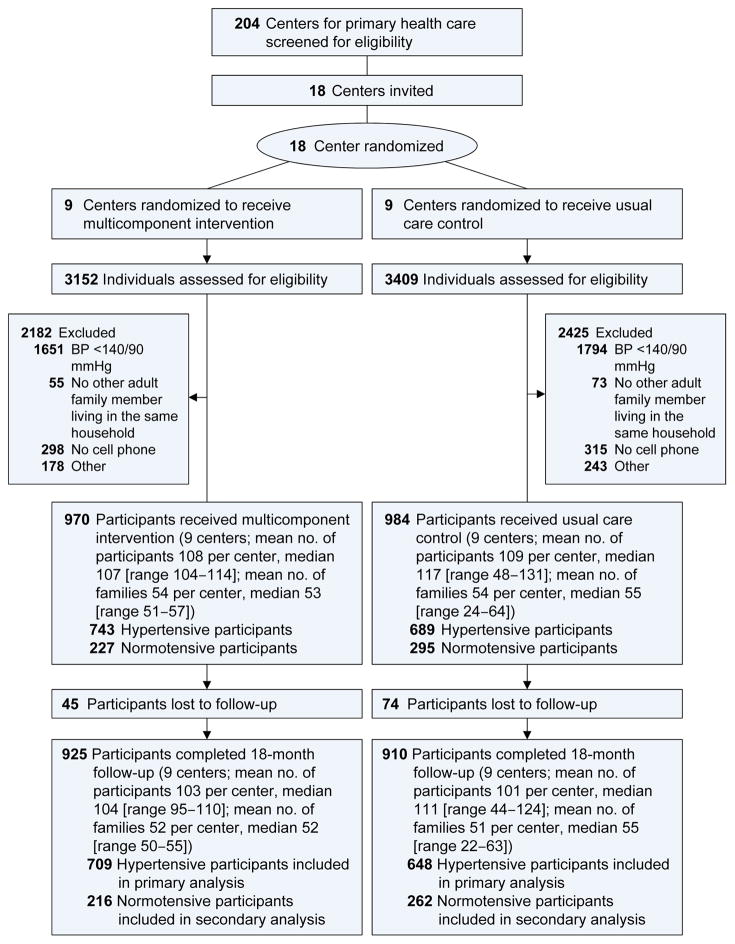
Design, setting, and participants: A cluster randomized trial was conducted in 18 centers for primary health care within a national public system providing free medications and health care to uninsured patients in Argentina. A total of 1432 low-income adult patients with uncontrolled hypertension were recruited between June 2013 and April 2015 and followed up to October 2016.
Interventions: Nine centers (743 patients) were randomized to the multicomponent intervention, which included a community health worker-led home intervention (health coaching, home BP monitoring, and BP audit and feedback), a physician intervention, and a text-messaging intervention over 18 months. Nine centers (689 patients) were randomized to usual care.
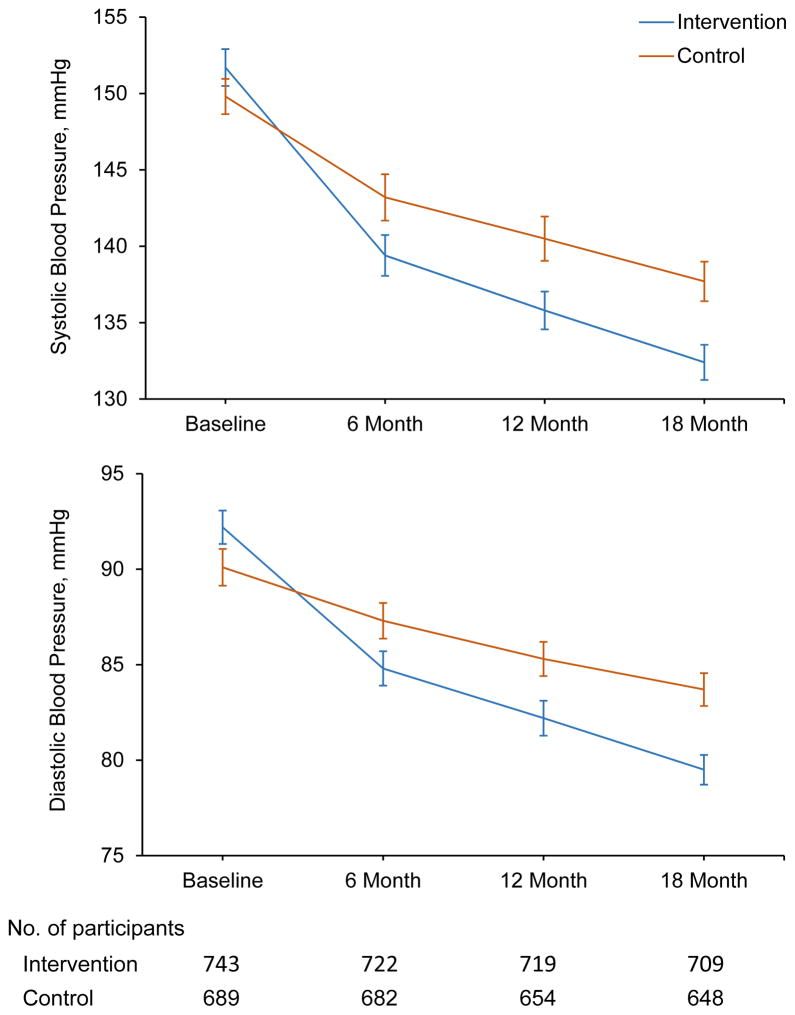
Main outcomes and measures: The coprimary outcomes were the differences in systolic and diastolic BP changes from baseline to the end of follow-up of patients with hypertension. Secondary outcomes included the proportion of patients with controlled hypertension (BP <140/90 mm Hg). Three BP measurements were obtained at each of 2 baseline and 2 termination visits using a standard protocol, the means of which were used for analyses.
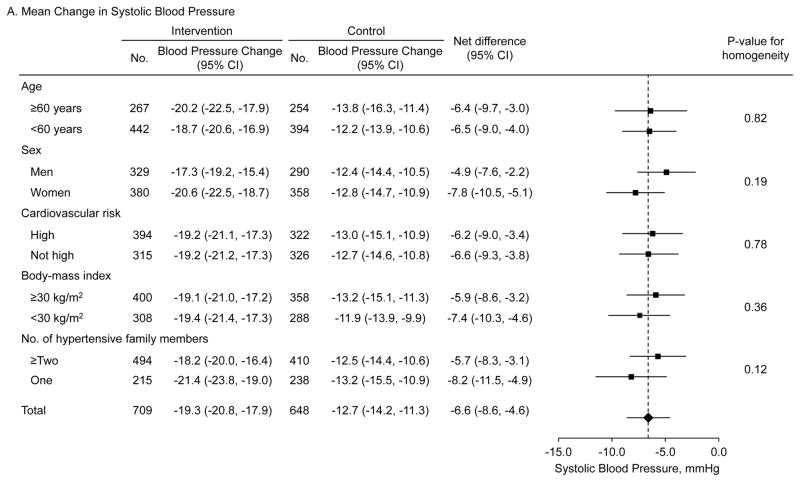
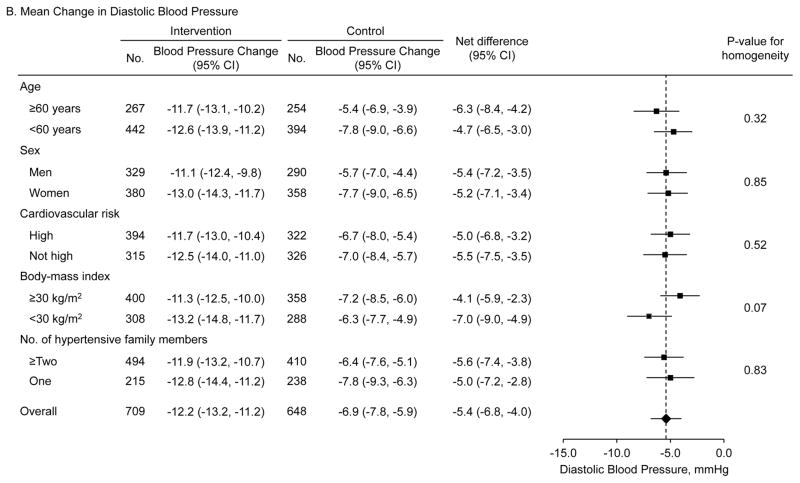
Results: Of 1432 participants (mean age, 55.8 years [SD, 13.3]; 772 women [53.0%]), 1357 (94.8%) completed the trial. Baseline mean systolic BP was 151.7 mm Hg for the intervention group and 149.8 mm Hg for the usual care group; the mean diastolic BP was 92.2 mm Hg for the intervention group and 90.1 mm Hg for the usual care group. Systolic BP reduction from baseline to month 18 was 19.3 mm Hg (95% CI, 17.9-20.8 mm Hg) for the intervention group and 12.7 mm Hg (95% CI, 11.3-14.2 mm Hg) for the usual care group; the difference in the reduction was 6.6 mm Hg (95% CI, 4.6-8.6; P < .001). Diastolic BP decreased by 12.2 mm Hg (95% CI, 11.2-13.2 mm Hg) in the intervention group and 6.9 mm Hg (95% CI, 5.9-7.8 mm Hg) in the control group; the difference in the reduction was 5.4 mm Hg (95% CI, 4.0-6.8 mm Hg; P < .001). The proportion of patients with controlled hypertension increased from 17.0% at baseline to 72.9% at 18 months in the intervention group and from 17.6% to 52.2% in the usual care group; the difference in the increase was 20.6% (95% CI, 15.4%-25.9%; P < .001). No adverse events were reported.
Conclusions and relevance: Low-income patients in Argentina with uncontrolled hypertension who participated in a community health worker-led multicomponent intervention experienced a greater decrease in systolic and diastolic BP than did patients who received usual care over 18 months. Further research is needed to assess generalizability and cost-effectiveness of this intervention and to understand which components may have contributed most to the outcome.
Trial registration: clinicaltrials.gov Identifier: NCT01834131.
Conflict of interest statement
Figures
Comment in
-
Improving Blood Pressure Control and Health Systems With Community Health Workers.JAMA. 2017 Sep 19;318(11):1009-1011. doi: 10.1001/jama.2017.11464. JAMA. 2017. PMID: 28975286 No abstract available.
References
-
- Forouzanfar MH, Liu P, Roth GA, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA. 2017;317(2):165–182. - PubMed
-
- He J, Gu D, Wu X, et al. Major causes of death among men and women in China. N Engl J Med. 2005;353(11):1124–34. - PubMed
-
- He J, Muntner P, Chen J, Roccella EJ, Streiffer RH, Whelton PK. Factors associated with hypertension control in the general population of the United States. Arch Intern Med. 2002;162(9):1051–8. - PubMed
-
- Odedosu T, Schoenthaler A, Vieira DL, Agyemang C, Ogedegbe G. Overcoming barriers to hypertension control in African Americans. Cleve Clin J Med. 2012;79(1):46–56. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
