

Adjuvant Chemotherapy vs Postoperative Observation Following Preoperative Chemoradiotherapy and Resection in Gastroesophageal Cancer: A Propensity Score-Matched Analysis
- PMID: 28975352
- PMCID: PMC5833647
- DOI: 10.1001/jamaoncol.2017.2805
Adjuvant Chemotherapy vs Postoperative Observation Following Preoperative Chemoradiotherapy and Resection in Gastroesophageal Cancer: A Propensity Score-Matched Analysis
Abstract
Importance: Distant recurrence following preoperative chemoradiotherapy and resection in patients with gastroesophageal adenocarcinoma is common. Adjuvant chemotherapy may improve survival.
Objective: To compare adjuvant chemotherapy with postoperative observation following preoperative chemoradiotherapy and resection in patients with gastroesophageal adenocarcinoma.
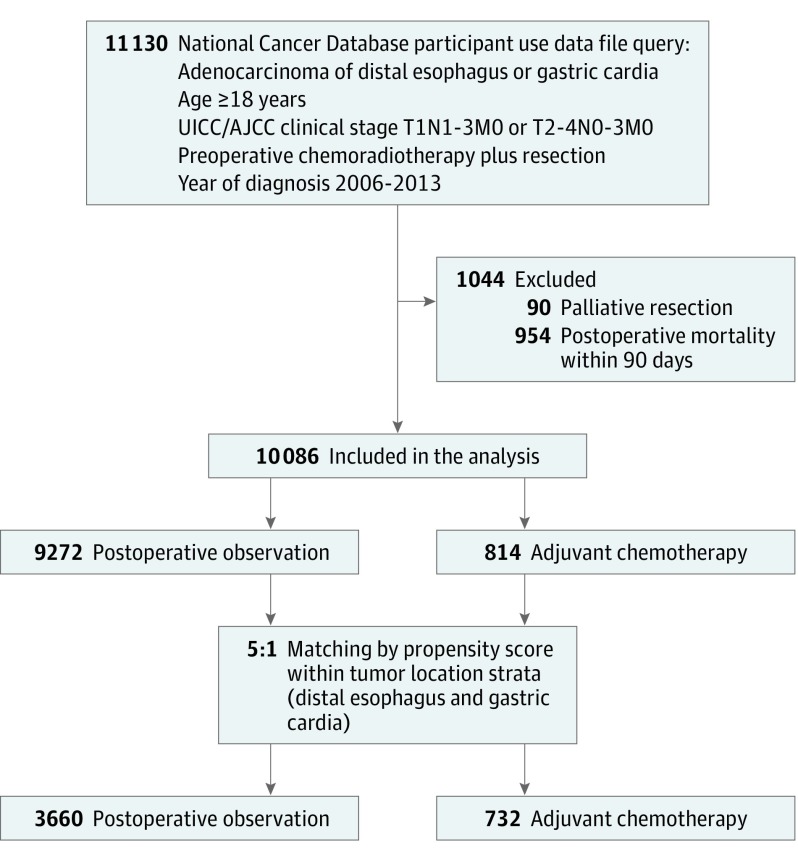
Design, setting, and participants: Propensity score-matched analysis using the National Cancer Database. We included adult patients who received a diagnosis between 2006 and 2013 of clinical stage T1N1-3M0 or T2-4N0-3M0 adenocarcinoma of the distal esophagus or gastric cardia who were treated with preoperative chemoradiotherapy and curative-intent resection. Patients receiving adjuvant chemotherapy were matched by propensity score to patients undergoing postoperative observation.
Exposures: Adjuvant chemotherapy and postoperative observation.
Main outcomes and measures: Overall survival.
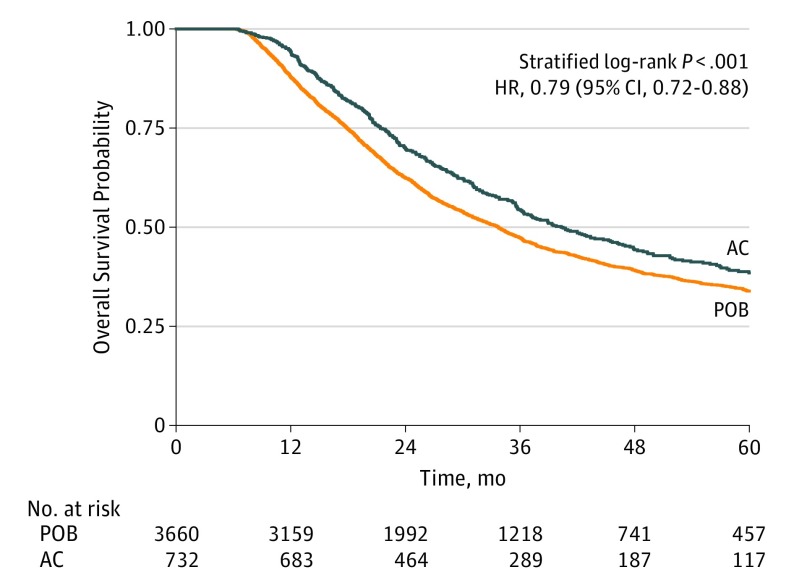
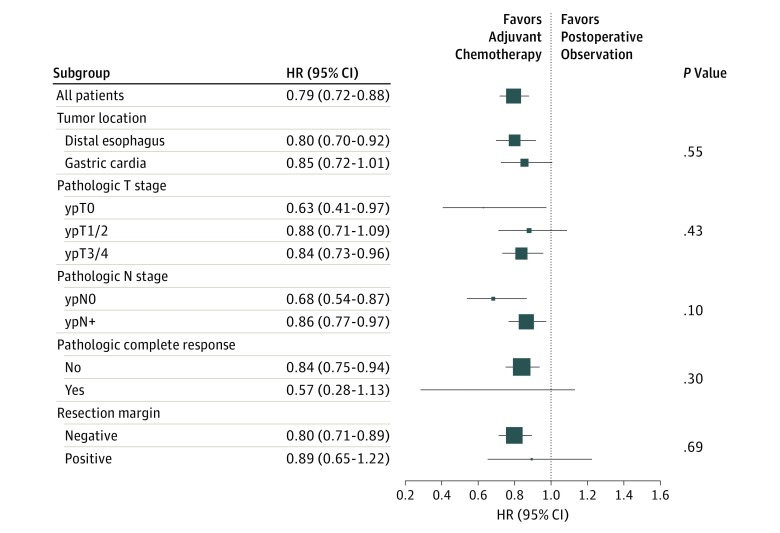
Results: We identified 10 086 patients (8840 [88%] male; mean [SD] age, 61 [9.5] years), 9272 in the postoperative observation group and 814 in the adjuvant chemotherapy group. Patients receiving adjuvant chemotherapy were younger (18-54 years: 252 [31%] vs 1989 [21%]; P < .001) and were more likely to have advanced disease (ypT3/4: 458 [62%] vs 3531 [46%]; P < .001; ypN+: 572 [72%] vs 3428 [39%]; P < .001), as well as shorter postoperative inpatient stays (>2 weeks: 94 [13%] vs 1589 [20%]; P < .001). A total of 732 patients in the adjuvant chemotherapy group were matched by propensity score to 3660 patients in the postoperative observation group. Adjuvant chemotherapy was associated with improved overall survival compared with postoperative observation (median survival: 40 months; 95% CI, 36-46 months vs 34 months; 95% CI, 32-35 months; stratified log-rank P < .001; hazard ratio, 0.79; 95% CI, 0.72-0.88). Overall survival at 1, 3, and 5 years was 88%, 47%, and 34% in the observation group, and 94%, 54%, and 38% in the adjuvant chemotherapy group, respectively. Adjuvant chemotherapy was associated with a survival benefit compared with postoperative observation in most patient subgroups.
Conclusions and relevance: For patients with locally advanced gastroesophageal adenocarcinoma treated with preoperative chemoradiotherapy and resection, adjuvant chemotherapy was associated with improved overall survival. Our findings have important implications for the postoperative treatment of this patient group for which few data are available.
Conflict of interest statement
Figures
Comment in
-
Adjuvant Chemotherapy Following Neoadjuvant Chemotherapy Plus Surgery for Patients With Gastroesophageal Cancer-Is There Room for Improvement?JAMA Oncol. 2018 Jan 1;4(1):38-39. doi: 10.1001/jamaoncol.2017.2792. JAMA Oncol. 2018. PMID: 28975190 Free PMC article. No abstract available.
References
-
- Stahl M, Walz MK, Stuschke M, et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol. 2009;27(6):851-856. - PubMed
-
- Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996;335(7):462-467. - PubMed
-
- van Hagen P, Hulshof MCCM, van Lanschot JJB, et al. ; CROSS Group . Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-2084. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
