

Robust intensity-modulated proton therapy to reduce high linear energy transfer in organs at risk
- PMID: 28976574
- PMCID: PMC5734644
- DOI: 10.1002/mp.12610
Robust intensity-modulated proton therapy to reduce high linear energy transfer in organs at risk
Abstract
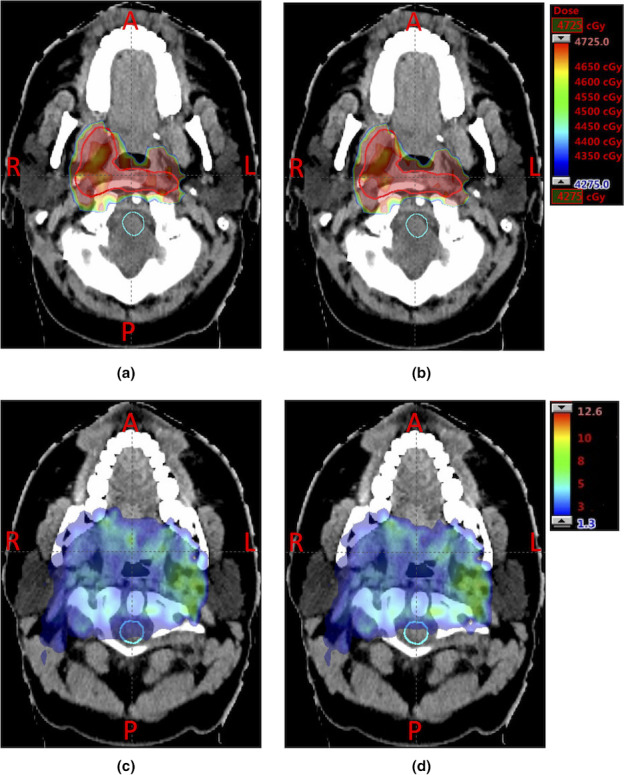
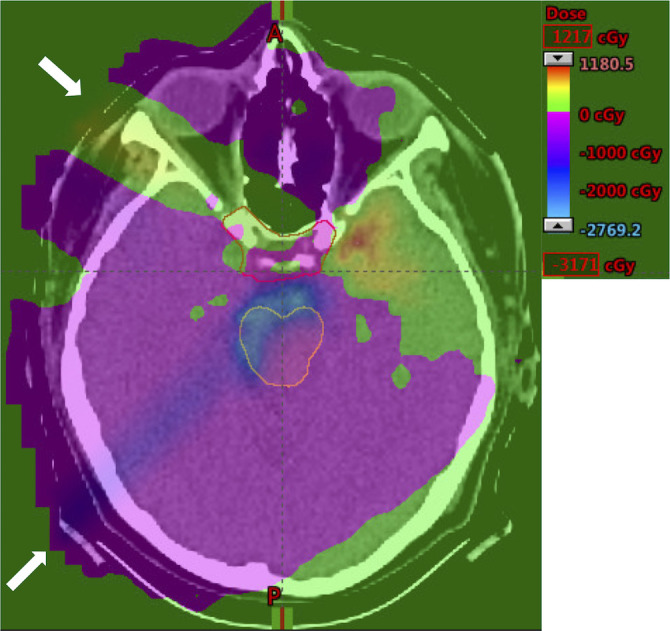
Purpose: We propose a robust treatment planning model that simultaneously considers proton range and patient setup uncertainties and reduces high linear energy transfer (LET) exposure in organs at risk (OARs) to minimize the relative biological effectiveness (RBE) dose in OARs for intensity-modulated proton therapy (IMPT). Our method could potentially reduce the unwanted damage to OARs.
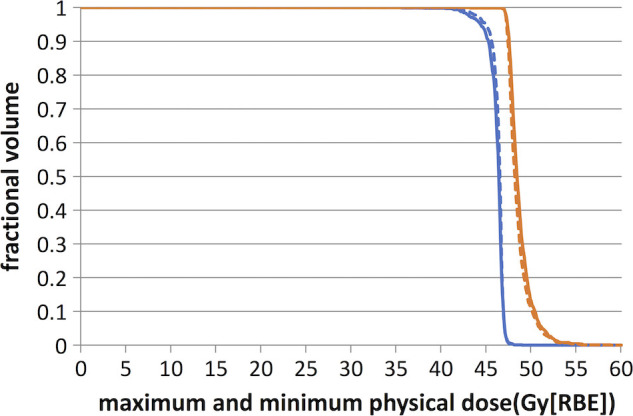
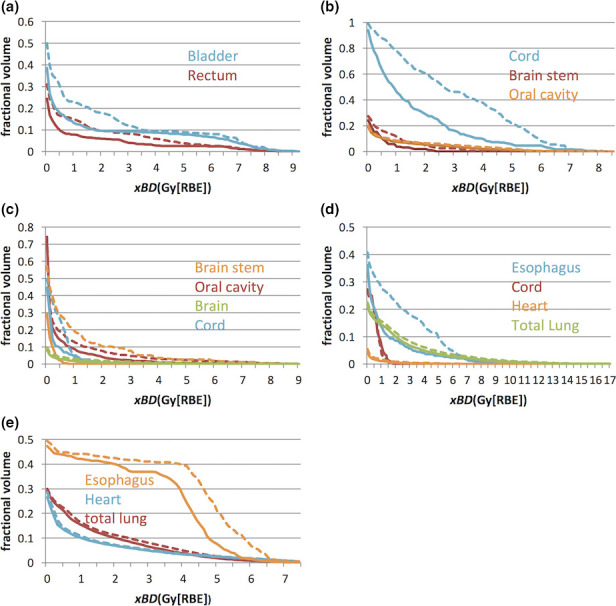
Methods: We retrospectively generated plans for 10 patients including two prostate, four head and neck, and four lung cancer patients. The "worst-case robust optimization" model was applied. One additional term as a "biological surrogate (BS)" of OARs due to the high LET-related biological effects was added in the objective function. The biological surrogate was defined as the sum of the physical dose and extra biological effects caused by the dose-averaged LET. We generated nine uncertainty scenarios that considered proton range and patient setup uncertainty. Corresponding to each uncertainty scenario, LET was obtained by a fast LET calculation method developed in-house and based on Monte Carlo simulations. In each optimization iteration, the model used the worst-case BS among all scenarios and then penalized overly high BS to organs. The model was solved by an efficient algorithm (limited-memory Broyden-Fletcher-Goldfarb-Shanno) in a parallel computing environment. Our new model was benchmarked with the conventional robust planning model without considering BS. Dose-volume histograms (DVHs) of the dose assuming a fixed RBE of 1.1 and BS for tumor and organs under nominal and uncertainty scenarios were compared to assess the plan quality between the two methods.
Results: For the 10 cases, our model outperformed the conventional robust model in avoidance of high LET in OARs. At the same time, our method could achieve dose distributions and plan robustness of tumors assuming a fixed RBE of 1.1 almost the same as those of the conventional robust model.
Conclusions: Explicitly considering LET in IMPT robust treatment planning can reduce the high LET to OARs and minimize the possible toxicity of high RBE dose to OARs without sacrificing plan quality. We believe this will allow one to design and deliver safer proton therapy.
Keywords: biological optimization; intensity-modulated proton therapy (IMPT); linear energy transfer (LET); robust optimization.
© 2017 American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare that they do not have any conflict of interest.
Figures
References
-
- Lim G, Cao W, Mohan R. Presented at the proceedings of the 15th asia pacific industrial engineering and management systems conference, pp 1520–1525, Jeju, Korea; 2014. (unpublished).
-
- Paganetti H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Phys Med Biol. 2014;59:R419. - PubMed
-
- Grassberger C, Paganetti H. Elevated LET components in clinical proton beams. Phys Med Biol. 2011;56:6677. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
