

Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: An individual participant data meta-analysis
- PMID: 28976987
- PMCID: PMC5627896
- DOI: 10.1371/journal.pmed.1002398
Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: An individual participant data meta-analysis
Abstract
Background: Babies born preterm are at an increased risk of dying in the first weeks of life, and those who survive have a higher rate of cerebral palsy (CP) compared with babies born at term. The aim of this individual participant data (IPD) meta-analysis (MA) was to assess the effects of antenatal magnesium sulphate, compared with no magnesium treatment, given to women at risk of preterm birth on important maternal and fetal outcomes, including survival free of CP, and whether effects differed by participant or treatment characteristics such as the reason the woman was at risk of preterm birth, why treatment was given, the gestational age at which magnesium sulphate treatment was received, or the dose and timing of the administration of magnesium sulphate.
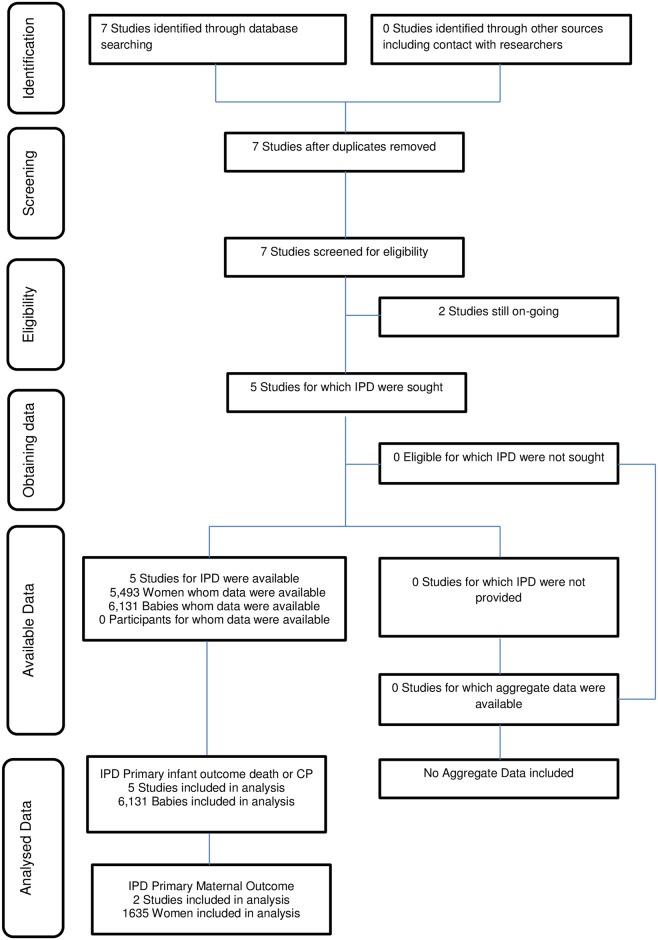
Methods and findings: Trials in which women considered at risk of preterm birth (<37 weeks' gestation) were randomised to magnesium sulphate or control treatment and where neurologic outcomes for the baby were reported were eligible for inclusion. The primary outcomes were infant death or CP and severe maternal outcome potentially related to treatment. Studies were identified based on the Cochrane Pregnancy and Childbirth search strategy using the terms [antenatal or prenatal] and [magnesium] and [preterm or premature or neuroprotection or 'cerebral palsy']. The date of the last search was 28 February 2017. IPD were sought from investigators with eligible trials. Risk of bias was assessed using criteria from the Cochrane Collaboration. For each prespecified outcome, IPD were analysed using a 1-stage approach. All 5 trials identified were included, with 5,493 women and 6,131 babies. Overall, there was no clear effect of magnesium sulphate treatment compared with no treatment on the primary infant composite outcome of death or CP (relative risk [RR] 0.94, 95% confidence interval (CI) 0.85 to 1.05, 6,131 babies, 5 trials, p = 0.07 for heterogeneity of treatment effect across trials). In the prespecified sensitivity analysis restricted to data from the 4 trials in which the intent of treatment was fetal neuroprotection, there was a significant reduction in the risk of death or CP with magnesium sulphate treatment compared with no treatment (RR 0.86, 95% CI 0.75 to 0.99, 4,448 babies, 4 trials), with no significant heterogeneity (p = 0.28). The number needed to treat (NNT) to benefit was 41 women/babies to prevent 1 baby from either dying or having CP. For the primary outcome of severe maternal outcome potentially related to magnesium sulphate treatment, no events were recorded from the 2 trials providing data. When the individual components of the composite infant outcome were assessed, no effect was seen for death overall (RR 1.03, 95% CI 0.91 to 1.17, 6,131 babies, 5 trials) or in the analysis of death using only data from trials with the intent of fetal neuroprotection (RR 0.95, 95% CI 0.80 to 1.13, 4,448 babies, 4 trials). For cerebral palsy in survivors, magnesium sulphate treatment had a strong protective effect in both the overall analysis (RR 0.68, 95% CI 0.54 to 0.87, 4,601 babies, 5 trials, NNT to benefit 46) and the neuroprotective intent analysis (RR 0.68, 95% CI 0.53 to 0.87, 3,988 babies, 4 trials, NNT to benefit 42). No statistically significant differences were seen for any of the other secondary outcomes. The treatment effect varied little by the reason the woman was at risk of preterm birth, the gestational age at which magnesium sulphate treatment was given, the total dose received, or whether maintenance therapy was used. A limitation of the study was that not all trials could provide the data required for the planned analyses so that combined with low event rates for some important clinical events, the power to find a difference was limited.
Conclusions: Antenatal magnesium sulphate given prior to preterm birth for fetal neuroprotection prevents CP and reduces the combined risk of fetal/infant death or CP. Benefit is seen regardless of the reason for preterm birth, with similar effects across a range of preterm gestational ages and different treatment regimens. Widespread adoption worldwide of this relatively inexpensive, easy-to-administer treatment would lead to important global health benefits for infants born preterm.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Magnesium sulfate prevents cerebral palsy in premature infants.J Pediatr. 2018 Mar;194:265-268. doi: 10.1016/j.jpeds.2017.12.079. J Pediatr. 2018. PMID: 29478499 No abstract available.
-
Antenatal magnesium sulfate treatment for women at risk of preterm birth is safe and might decrease the risk of cerebral palsy.BMJ Evid Based Med. 2018 Oct;23(5):195-196. doi: 10.1136/bmjebm-2018-110897. Epub 2018 Jun 19. BMJ Evid Based Med. 2018. PMID: 29921710 No abstract available.
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012;379(9832):2162–72. doi: 10.1016/S0140-6736(12)60820-4 - DOI - PubMed
-
- Chow SSW, Le Marsney R, Hossain S, Haslam R, Lui K. 2015. Report of the Australian and New Zealand Neonatal Network 2013. Sydney.
-
- World Health Organization. WHO recommendations on interventions to improve preterm birth outcomes. Geneva: WHO; 2015. - PubMed
-
- Saigal S, Doyle LW: An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008;371(9608):261–269. doi: 10.1016/S0140-6736(08)60136-1 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
