

Incidence of DAA failure and the clinical impact of retreatment in real-life patients treated in the advanced stage of liver disease: Interim evaluations from the PITER network
- PMID: 28977040
- PMCID: PMC5627924
- DOI: 10.1371/journal.pone.0185728
Incidence of DAA failure and the clinical impact of retreatment in real-life patients treated in the advanced stage of liver disease: Interim evaluations from the PITER network
Abstract
Background: Few data are available on the virological and clinical outcomes of advanced liver disease patients retreated after first-line DAA failure.
Aim: To evaluate DAA failure incidence and the retreatment clinical impact in patients treated in the advanced liver disease stage.
Methods: Data on HCV genotype, liver disease severity, and first and second line DAA regimens were prospectively collected in consecutive patients who reached the 12-week post-treatment and retreatment evaluations from January 2015 to December 2016 in 23 of the PITER network centers.
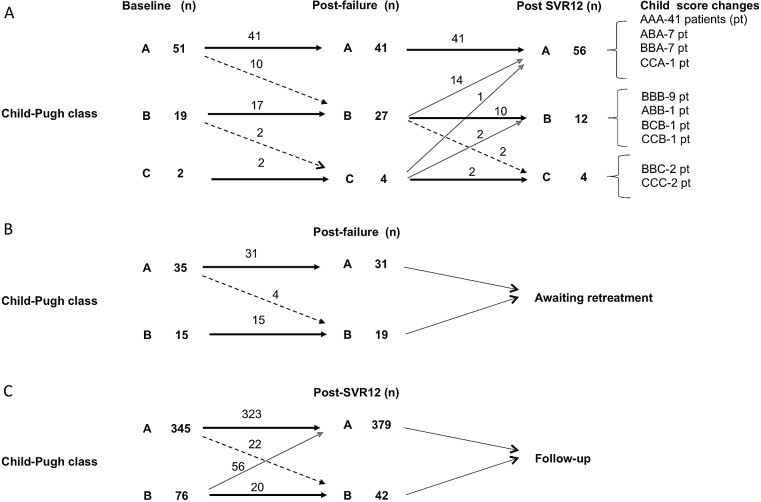
Results: Among 3,830 patients with advanced fibrosis (F3) or cirrhosis, 139 (3.6%) failed to achieve SVR. Genotype 3, bilirubin levels >1.5mg/dl, platelet count <120,000/mm3 and the sofosbuvir+ribavirin regimen were independent predictors of failure by logistic regression analysis. The failure rate was 7.6% for patients treated with regimens that are no longer recommended or considered suboptimal (sofosbuvir+ribavirin or simeprevir+sofosbuvir±ribavirin), whereas 1.4% for regimens containing sofosbuvir combined with daclatasvir or ledipasvir or other DAAs. Of the patients who failed to achieve SVR, 72 (51.8%) were retreated with a second DAA regimen, specifically 38 (52.7%) with sofosbuvir+daclatasvir, 27 (37.5%) with sofosbuvir+ledipasvir, and 7 (9.7%) with other DAAs ±ribavirin. Among these, 69 (96%) patients achieved SVR12 and 3 (4%) failed. During a median time of 6 months (range: 5-14 months) between failure and the second DAA therapy, the Child-Pugh class worsened in 12 (16.7%) patients: from A to B in 10 patients (19.6%) and from B to C in 2 patients (10.5%), whereas it did not change in the remaining 60 patients. Following the retreatment SVR12 (median time of 6 months; range: 3-12 months), the Child-Pugh class improved in 17 (23.6%) patients: from B to A in 14 (19.4%) patients, from C to A in 1 patient (1.4%) and from C to B in 2 (2.9%) patients; it remained unchanged in 53 patients (73.6%) and worsened in 2 (2.8%) patients. Of patients who were retreated, 3 (4%) had undergone OLT before retreatment (all reached SVR12 following retreatment) and 2 (2.8%) underwent OLT after having achieved retreatment SVR12. Two (70%) of the 3 patients who failed to achieve SVR12 after retreatment, and 2 (2.8%) of the 69 patients who achieved retreatment SVR12 died from liver failure (Child-Pugh class deteriorated from B to C) or HCC complications.
Conclusions: Failure rate following the first DAA regimen in patients with advanced disease is similar to or lower than that reported in clinical trials, although the majority of patients were treated with suboptimal regimens. Interim findings showed that worsening of liver function after failure, in terms of Child Pugh class deterioration, was improved by successful retreatment in about one third of retreated patients within a short follow-up period; however, in some advanced liver disease patients, clinical outcomes (Child Pugh class, HCC development, liver failure and death) were independent of viral eradication.
Conflict of interest statement
Figures
References
-
- WHO. Hepatitis C. Fact sheet updated April 2017. Available from: http://www.who.int/mediacentre/factsheets/fs164/en/
-
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis 2005;5: 558–567. doi: 10.1016/S1473-3099(05)70216-4 - DOI - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380: 2095–2128. doi: 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- WHO. Global health sector strategy on viral hepatitis 2016–2021. Available from http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/
-
- George SL, Bacon BR, Brunt EM, Mihindukulasuriya KL,Hoffmann J, Di Bisceglie AM. Clinical, virologic, histologic, and biochemical outcomes after successful HCV therapy: a 5-year follow-up of 150 patients. Hepatology. 2009; 49:729–738. doi: 10.1002/hep.22694 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
