

Population trends in the incidence and initial management of osteoarthritis: age-period-cohort analysis of the Clinical Practice Research Datalink, 1992-2013
- PMID: 28977564
- PMCID: PMC5850125
- DOI: 10.1093/rheumatology/kex270
Population trends in the incidence and initial management of osteoarthritis: age-period-cohort analysis of the Clinical Practice Research Datalink, 1992-2013
Abstract
Objective: To determine recent trends in the rate and management of new cases of OA presenting to primary healthcare using UK nationally representative data.
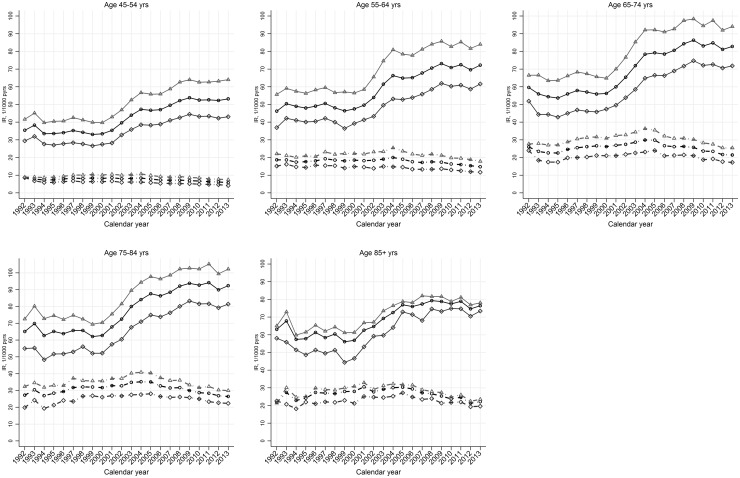
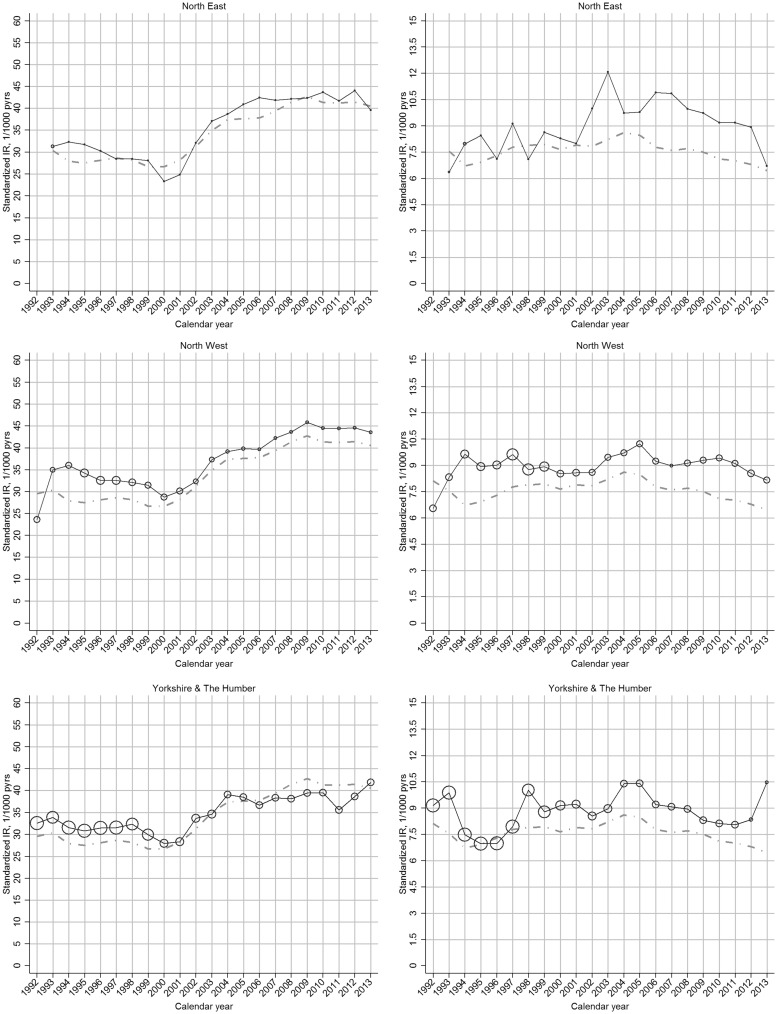
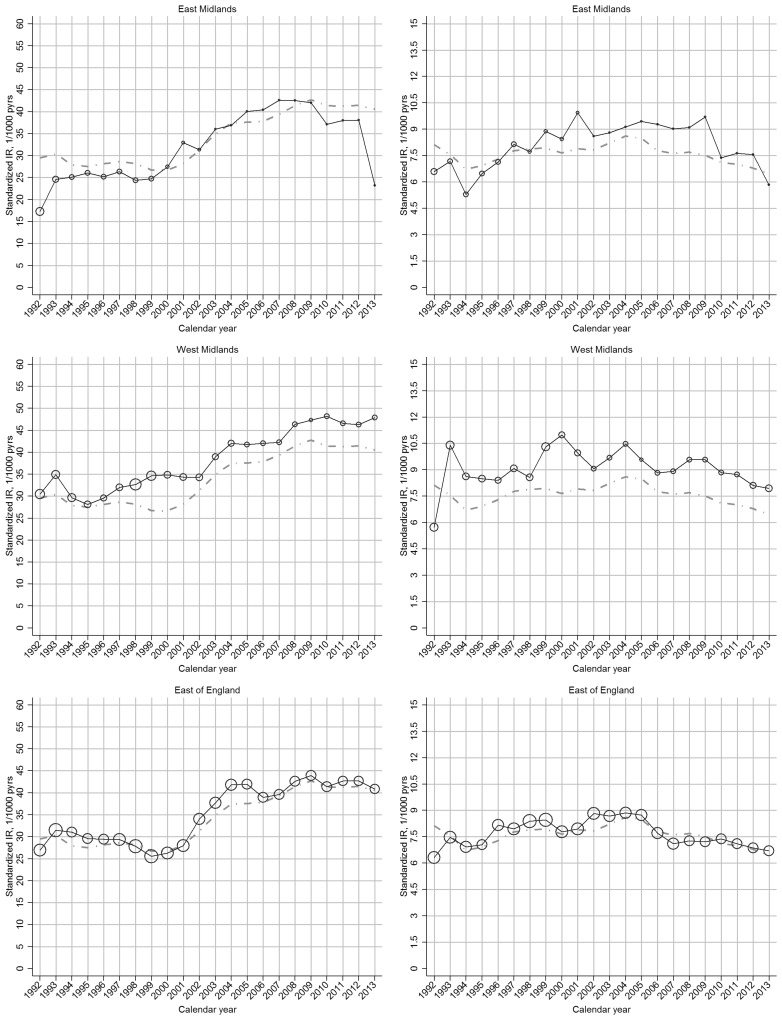
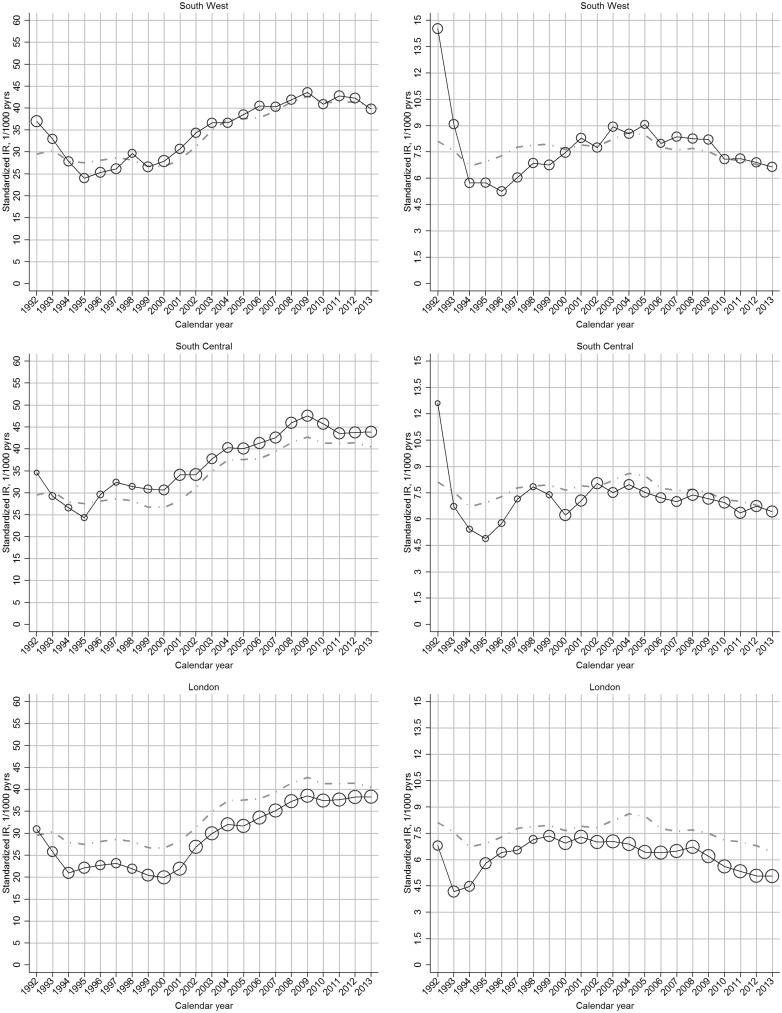
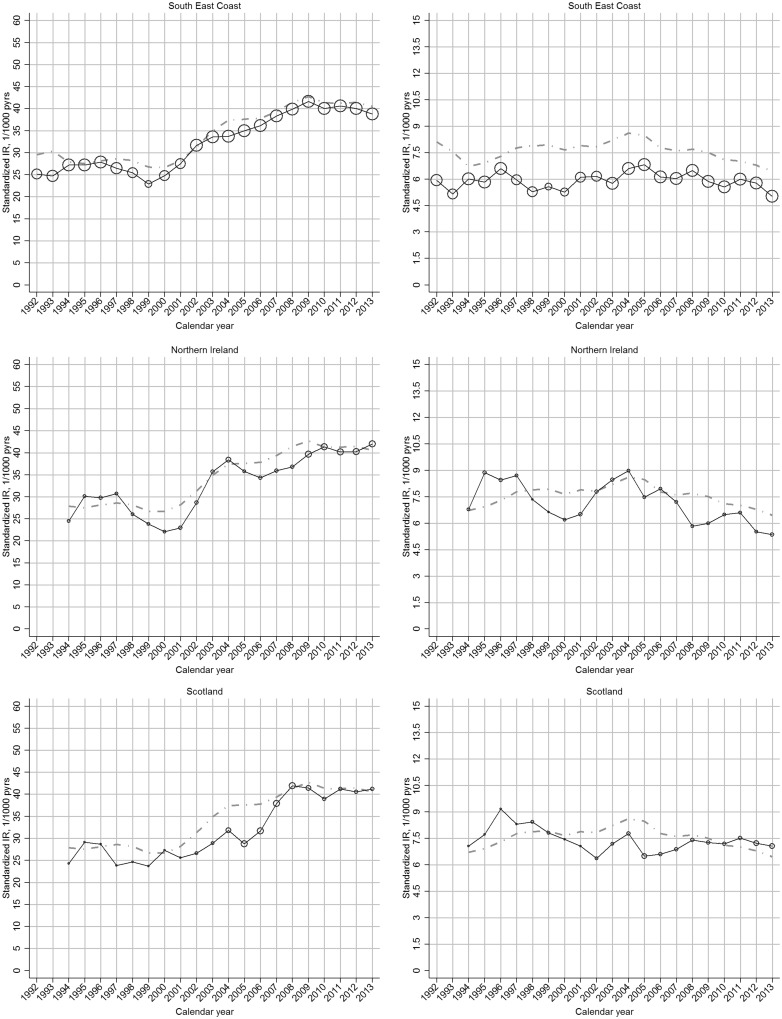
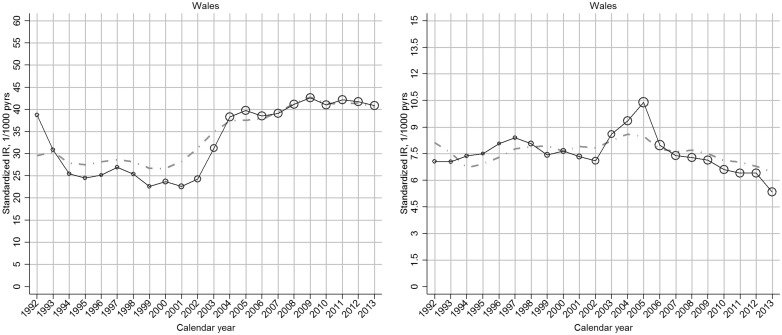
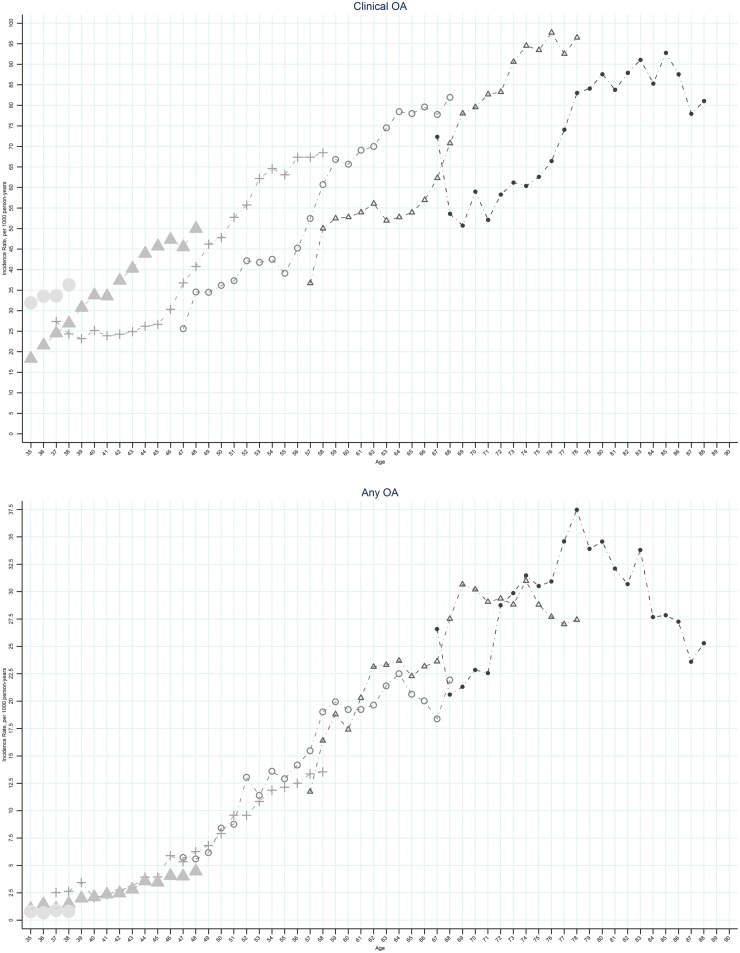
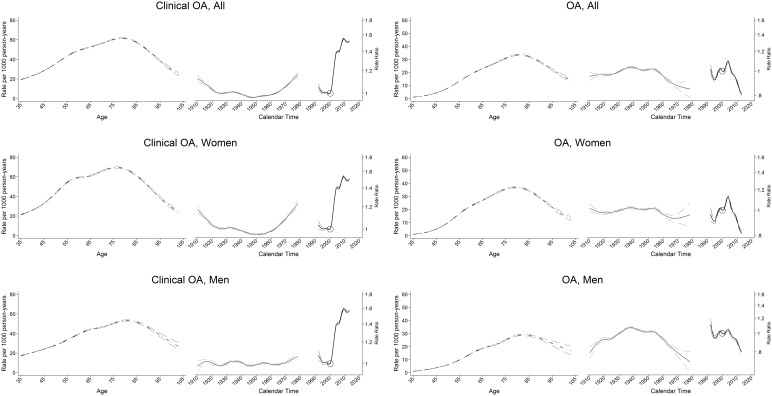
Methods: Using the Clinical Practice Research Datalink we identified new cases of diagnosed OA and clinical OA (including OA-relevant peripheral joint pain in those aged over 45 years) using established code lists. For both definitions we estimated annual incidence density using exact person-time, and undertook descriptive analysis and age-period-cohort modelling. Demographic characteristics and management were described for incident cases in each calendar year. Sensitivity analyses explored the robustness of the findings to key assumptions.
Results: Between 1992 and 2013 the annual age-sex standardized incidence rate for clinical OA increased from 29.2 to 40.5/1000 person-years. After controlling for period effects, the consultation incidence of clinical OA was higher for successive cohorts born after the mid-1950s, particularly women. In contrast, with the exception of hand OA, we observed no increase in the incidence of diagnosed OA: 8.6/1000 person-years in 2004 down to 6.3 in 2013. In 2013, 16.4% of clinical OA cases had an X-ray referral. While NSAID prescriptions fell from 2004, the proportion prescribed opioid analgesia rose markedly (0.1% of diagnosed OA in 1992 to 1.9% in 2013).
Conclusion: Rising rates of clinical OA, continued use of plain radiography and a shift towards opioid analgesic prescription are concerning. Our findings support the search for policies to tackle this common problem that promote joint pain prevention while avoiding excessive and inappropriate health care.
Keywords: analgesics; incidence; osteoarthritis; primary care.
© The Author 2017. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
Comment in
-
Therapy: Are you managing osteoarthritis appropriately?Nat Rev Rheumatol. 2017 Dec;13(12):703-704. doi: 10.1038/nrrheum.2017.160. Epub 2017 Sep 21. Nat Rev Rheumatol. 2017. PMID: 28931953 No abstract available.
References
-
- Pabinger C, Geissler A.. Utilization rates of hip arthroplasty in OECD countries. Osteoarthritis Cartilage 2014;22:734–41. - PubMed
-
- Pabinger C, Lothaller H, Geissler A.. Utilization rates of knee-arthroplasty in OECD countries. Osteoarthritis Cartilage 2015;23:1664–73. - PubMed
-
- Culliford DJ, Maskell J, Beard DJ. et al. Temporal trends in hip and knee replacement in the United Kingdom: 1991 to 2006. J Bone Joint Surg Br 2010;92:130–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
