

Imatinib in systemic mastocytosis: a phase IV clinical trial in patients lacking exon 17 KIT mutations and review of the literature
- PMID: 28978170
- PMCID: PMC5620310
- DOI: 10.18632/oncotarget.10711
Imatinib in systemic mastocytosis: a phase IV clinical trial in patients lacking exon 17 KIT mutations and review of the literature
Abstract
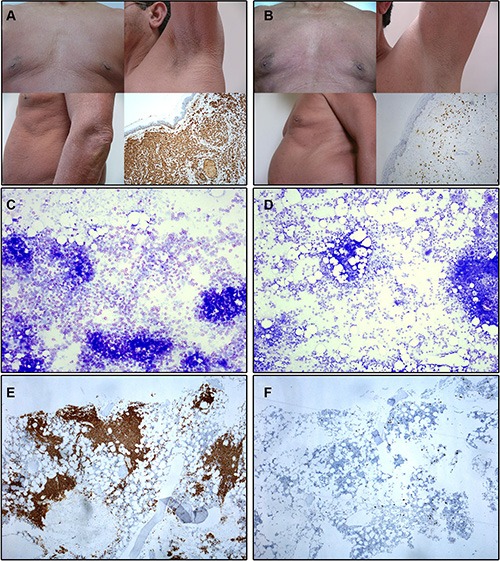
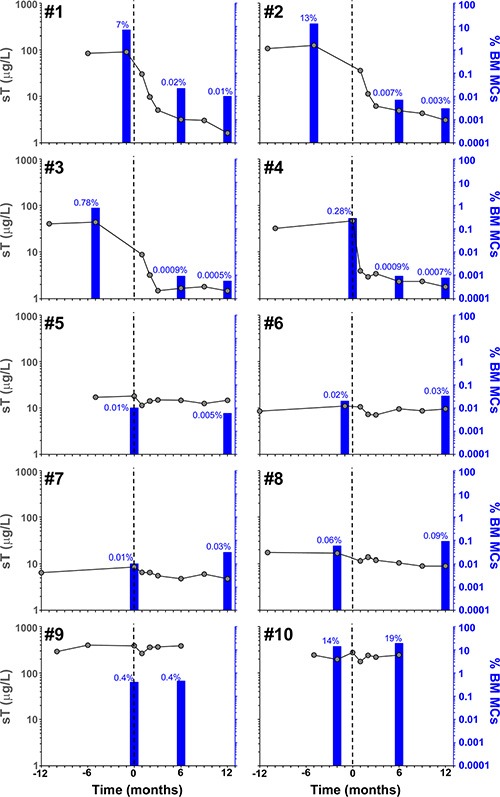
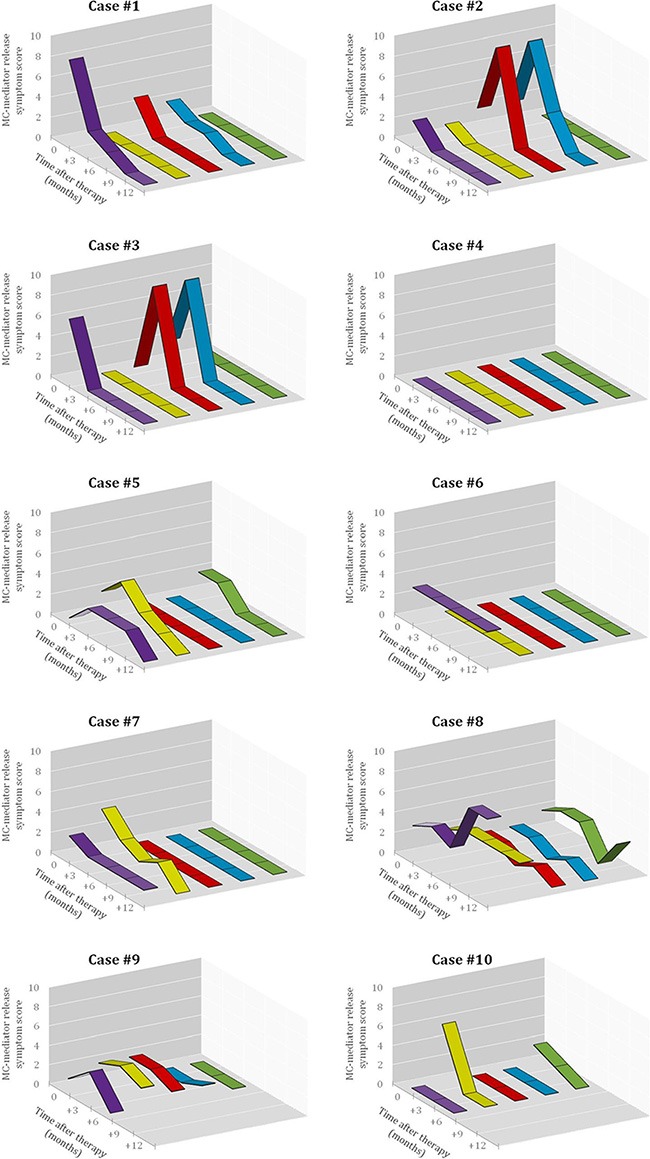
Resistance to imatinib has been recurrently reported in systemic mastocytosis (SM) carrying exon 17 KIT mutations. We evaluated the efficacy and safety of imatinib therapy in 10 adult SM patients lacking exon 17 KIT mutations, 9 of which fulfilled criteria for well-differentiated SM (WDSM). The World Health Organization 2008 disease categories among WDSM patients were mast cell (MC) leukemia (n = 3), indolent SM (n = 3) and cutaneous mastocytosis (n = 3); the remainder case had SM associated with a clonal haematological non-MC disease. Patients were given imatinib for 12 months -400 or 300 mg daily depending on the presence vs. absence of > 30% bone marrow (BM) MCs and/or signs of advanced disease-. Absence of exon 17 KIT mutations was confirmed in highly-purified BM MCs by peptide nucleic acid-mediated PCR, while mutations involving other exons were investigated by direct sequencing of purified BM MC DNA. Complete response (CR) was defined as resolution of BM MC infiltration, skin lesions, organomegalies and MC-mediator release-associated symptoms, plus normalization of serum tryptase. Criteria for partial response (PR) included ≥ 50% reduction in BM MC infiltration and improvement of skin lesions and/or organomegalies. Treatment was well-tolerated with an overall response rate of 50%, including early and sustained CR in four patients, three of whom had extracellular mutations of KIT, and PR in one case. This later patient and all non-responders (n = 5) showed wild-type KIT. These results together with previous data from the literature support the relevance of the KIT mutational status in selecting SM patients who are candidates for imatinib therapy.
Keywords: KIT; imatinib; mast cell; mastocytosis; well-differentiated systemic mastocytosis.
Conflict of interest statement
CONFLICTS OF INTEREST The authors declare no competing financial interest.
Figures
Similar articles
-
Clinical, immunophenotypic, and molecular characteristics of well-differentiated systemic mastocytosis.J Allergy Clin Immunol. 2016 Jan;137(1):168-178.e1. doi: 10.1016/j.jaci.2015.05.008. Epub 2015 Jun 19. J Allergy Clin Immunol. 2016. PMID: 26100086
-
Mastocytosis: state of the art.Pathobiology. 2007;74(2):121-32. doi: 10.1159/000101711. Pathobiology. 2007. PMID: 17587883 Review.
-
Long-lasting complete response to imatinib in a patient with systemic mastocytosis exhibiting wild type KIT.Am J Blood Res. 2014 Dec 15;4(2):93-100. eCollection 2014. Am J Blood Res. 2014. PMID: 25755909 Free PMC article.
-
Nonaggressive systemic mastocytosis (SM) without skin lesions associated with insect-induced anaphylaxis shows unique features versus other indolent SM.J Allergy Clin Immunol. 2014 Feb;133(2):520-8. doi: 10.1016/j.jaci.2013.06.020. Epub 2013 Aug 6. J Allergy Clin Immunol. 2014. PMID: 23921094
-
Venom immunotherapy in patients with mastocytosis and hymenoptera venom anaphylaxis.Immunotherapy. 2011 May;3(5):637-51. doi: 10.2217/imt.11.44. Immunotherapy. 2011. PMID: 21554093 Review.
Cited by
-
Poor Applicability of Currently Available Prognostic Scoring Systems for Prediction of Outcome in KIT D816V-Negative Advanced Systemic Mastocytosis.Cancers (Basel). 2024 Jan 30;16(3):593. doi: 10.3390/cancers16030593. Cancers (Basel). 2024. PMID: 38339343 Free PMC article.
-
Comparative oncology: The paradigmatic example of canine and human mast cell neoplasms.Vet Comp Oncol. 2019 Mar;17(1):1-10. doi: 10.1111/vco.12440. Epub 2018 Sep 24. Vet Comp Oncol. 2019. PMID: 30136349 Free PMC article. Review.
-
c-Kit Receptors as a Therapeutic Target in Cancer: Current Insights.Onco Targets Ther. 2023 Sep 27;16:785-799. doi: 10.2147/OTT.S404648. eCollection 2023. Onco Targets Ther. 2023. PMID: 37790582 Free PMC article. Review.
-
Preclinical human models and emerging therapeutics for advanced systemic mastocytosis.Haematologica. 2018 Nov;103(11):1760-1771. doi: 10.3324/haematol.2018.195867. Epub 2018 Jul 5. Haematologica. 2018. PMID: 29976735 Free PMC article. Review.
-
A Rare Case of Acute Aleukemic Mast Cell Leukemia With Osteoblastic Lesions in the Appendicular Skeleton.J Hematol. 2025 Feb;14(1):32-37. doi: 10.14740/jh1383. Epub 2025 Jan 17. J Hematol. 2025. PMID: 39935699 Free PMC article.
References
-
- Horny HP, Metcalfe DD, Bennet JM, Bain BJ, Akin C, Escribano L, Valent P, Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. Mastocytosis. In: Swerdlow SH, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon: IARC; 2008. pp. 54–63.
-
- Escribano L, Orfao A, Villarrubia J, Díaz-Agustin B, Cerveró C, Ríos A, Velasco JL, Ciudad J, Navarro JL, San Miguel JF. Immunophenotypic characterization of human bone marrow mast cells. A flow cytometric study of normal and pathological bone marrow samples. An Cell Pathol. 1998;16:151–159. - PMC - PubMed
-
- Escribano L, Díaz Agustín B, Bravo P, Navalón R, Almeida J, Orfao A. Immunophenotype of Bone Marrow Mast Cells in Indolent Systemic Mast Cell Disease in Adults. Leuk Lymphoma. 1999;35:227–235. - PubMed
-
- Garcia-Montero AC, Jara-Acevedo M, Teodosio C, Sanchez ML, Nunez R, Prados A, Aldanondo I, Sanchez L, Dominguez M, Botana LM, Sanchez-Jimenez F, Sotlar K, Almeida J, et al. KIT mutation in mast cells and other bone marrow haematopoietic cell lineages in systemic mast cell disorders. A prospective study of the Spanish Network on Mastocytosis (REMA) in a series of 113 patients. Blood. 2006;108:2366–2372. - PubMed
-
- Kristensen T, Vestergaard H, Bindslev-Jensen C, Møller M, Broesby-Olsen S. Sensitive KIT D816V mutation analysis of blood as a diagnostic test in mastocytosis. Am J Hematol. 2014;89:493–498. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
