

Rehabilitation for Shoulder Instability - Current Approaches
- PMID: 28979601
- PMCID: PMC5611703
- DOI: 10.2174/1874325001711010957
Rehabilitation for Shoulder Instability - Current Approaches
Abstract
Background: The shoulder relies predominantly on dynamic muscular control to provide stability. Successful treatment is highly dependent upon the correct clinical diagnosis, identification of anatomical structural defects and abnormal movement patterns so that rehabilitation programs can be designed accordingly and individualised to the patient.
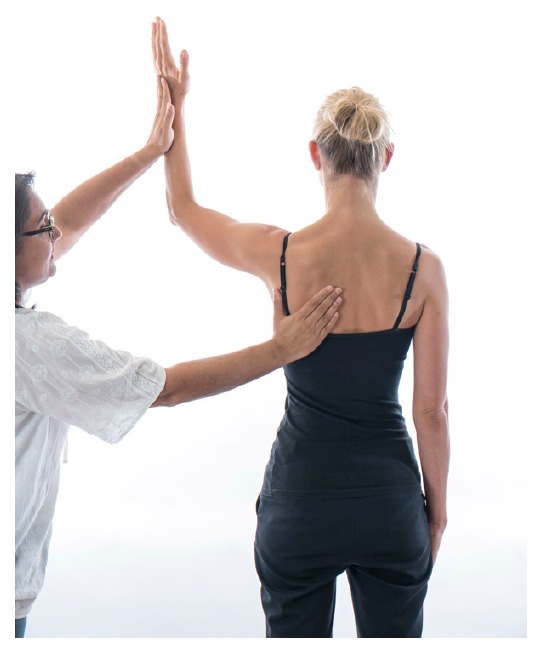
Method: A systematic outline is provided to guide the clinician on how to identify muscular insufficiencies both local to the shoulder joint and global muscles that can influence shoulder instability. Management is based on expert experience and current literature.
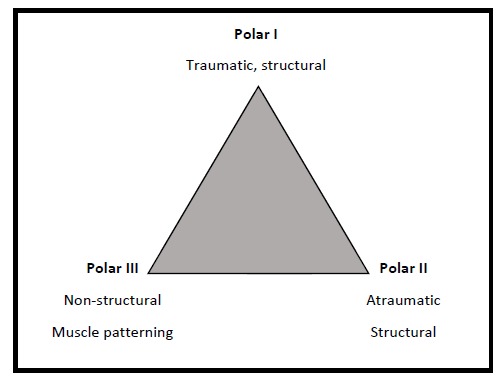
Results: The Stanmore classification helps to correctly diagnose the type of instability and prioritise management. Symptom modification tests can help to guide management, however assessing individual muscle groups local to glenohumeral control is also recommended.
Conclusion: Physical and psychosocial factors can influence motor control in the presence of pain and injury. A multi-disciplinary approach is required to avoid recurrence of symptoms with rehabilitation focusing on kinetic chain, scapular and gleno-humeral control.
Keywords: Assessment; Exercise; Instability; Rehabilitation; Rotator Cuff; Shoulder.
Figures









References
-
- Lewis A., Kitamura T., Bayley J.I. Mini symposium: shoulder instability (ii) The classification of shoulder instability: New light through old windows. Curr. Orthop. 2004;18:97–108. doi: 10.1016/j.cuor.2004.04.002. - DOI
-
- Robinson C.M., Howes J., Murdoch H., Will E., Graham C. Functional outcome and risk of recurrent instability after primary traumatic anterior shoulder dislocation in young patients. J. Bone Joint Surg. Am. 2006;88(11):2326–2336. - PubMed
-
- McAuliffe T.B., Pangayatselvan T., Bayley I. Failed surgery for recurrent anterior dislocation of the shoulder. Causes and management. J. Bone Joint Surg. Br. 1988;70(5):798–801. - PubMed
-
- Malone A.A., Jaggi A., Calvert P.T., et al. Muscle patterning instability – classification and prevalence in reference shoulder service. In: Norris T.R., Zuckerman J.D., Warner J.J., Lee Q.T., editors. Surgery of the shoulder and elbow: an international perspective. Illinois, USA: American Academy of Orthopaedic Surgeons; 2006.
-
- Jaggi A., Alexander S., Herbert R., Funk L., Ginn K.A. Does surgery followed by physiotherapy improve short and long term outcome for patients with atraumatic shoulder instability compared with physiotherapy alone? protocol for a randomized controlled clinical trial. BMC Musculoskelet. Disord. 2014;15:439. doi: 10.1186/1471-2474-15-439. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources