

Comparison of Simulated Treatment and Cost-effectiveness of a Stepped Care Case-Finding Intervention vs Usual Care for Posttraumatic Stress Disorder After a Natural Disaster
- PMID: 28979968
- PMCID: PMC6583387
- DOI: 10.1001/jamapsychiatry.2017.3037
Comparison of Simulated Treatment and Cost-effectiveness of a Stepped Care Case-Finding Intervention vs Usual Care for Posttraumatic Stress Disorder After a Natural Disaster
Abstract
Importance: Psychiatric interventions offered after natural disasters commonly address subsyndromal symptom presentations, but often remain insufficient to reduce the burden of chronic posttraumatic stress disorder (PTSD).
Objective: To simulate a comparison of a stepped care case-finding intervention (stepped care [SC]) vs a moderate-strength single-level intervention (usual care [UC]) on treatment effectiveness and incremental cost-effectiveness in the 2 years after a natural disaster.
Design, setting, and participants: This study, which simulated treatment scenarios that start 4 weeks after landfall of Hurricane Sandy on October 29, 2012, and ending 2 years later, created a model of 2 642 713 simulated agents living in the areas of New York City affected by Hurricane Sandy.
Interventions: Under SC, cases were referred to cognitive behavioral therapy, an evidence-based therapy that aims to improve symptoms through problem solving and by changing thoughts and behaviors; noncases were referred to Skills for Psychological Recovery, an evidence-informed therapy that aims to reduce distress and improve coping and functioning. Under UC, all patients were referred only to Skills for Psychological Recovery.
Main outcomes and measures: The reach of SC compared with UC for 2 years, the 2-year reduction in prevalence of PTSD among the full population, the 2-year reduction in the proportion of PTSD cases among initial cases, and 10-year incremental cost-effectiveness.
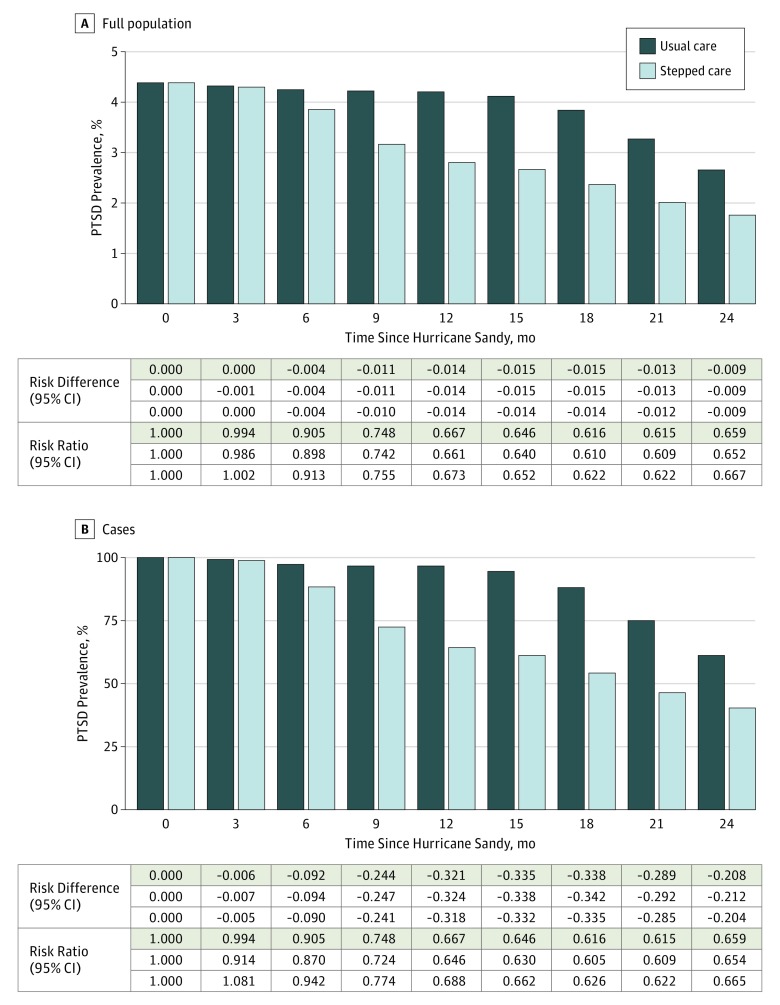
Results: This population of 2 642 713 simulated agents was initialized with a PTSD prevalence of 4.38% (115 751 cases) and distributions of sex (52.6% female and 47.4% male) and age (33.9% aged 18-34 years, 49.0% aged 35-64 years, and 17.1% aged ≥65 years) that were comparable with population estimates in the areas of New York City affected by Hurricane Sandy. Stepped care was associated with greater reach and was superior to UC in reducing the prevalence of PTSD in the full population: absolute benefit was clear at 6 months (risk difference [RD], -0.004; 95% CI, -0.004 to -0.004), improving through 1.25 years (RD, -0.015; 95% CI, -0.015 to -0.014). Relative benefits of SC were clear at 6 months (risk ratio, 0.905; 95% CI, 0.898-0.913), with continued gains through 1.75 years (risk ratio, 0.615; 95% CI, 0.609-0.662). The absolute benefit of SC among cases was much stronger, emerging at 3 months (RD, -0.006; 95% CI, -0.007 to -0.005) and increasing through 1.5 years (RD, -0.338; 95% CI, -0.342 to -0.335). Relative benefits of SC among cases were equivalent to those observed in the full population. The incremental cost-effectiveness of SC compared with UC was $3428.71 to $6857.68 per disability-adjusted life year avoided, and $0.80 to $1.61 per PTSD-free day.
Conclusions and relevance: The results of this simulation study suggest that SC for individuals with PTSD in the aftermath of a natural disaster is associated with greater reach than UC, more effectiveness than UC, and is well within the range of acceptability for cost-effectiveness. Results should be considered in light of limitations inherent to agent-based models.
Conflict of interest statement
Figures


Similar articles
-
Effectiveness of Group Problem Management Plus, a brief psychological intervention for adults affected by humanitarian disasters in Nepal: A cluster randomized controlled trial.PLoS Med. 2021 Jun 17;18(6):e1003621. doi: 10.1371/journal.pmed.1003621. eCollection 2021 Jun. PLoS Med. 2021. PMID: 34138875 Free PMC article. Clinical Trial.
-
Centrally Assisted Collaborative Telecare for Posttraumatic Stress Disorder and Depression Among Military Personnel Attending Primary Care: A Randomized Clinical Trial.JAMA Intern Med. 2016 Jul 1;176(7):948-56. doi: 10.1001/jamainternmed.2016.2402. JAMA Intern Med. 2016. PMID: 27294447 Clinical Trial.
-
Alcohol and Nonmedical Prescription Drug Use to Cope With Posttraumatic Stress Disorder Symptoms: An Analysis of Hurricane Sandy Survivors.Subst Use Misuse. 2017 Aug 24;52(10):1348-1356. doi: 10.1080/10826084.2017.1280832. Epub 2017 Apr 10. Subst Use Misuse. 2017. PMID: 28394737
-
Psychological therapies for the treatment of post-traumatic stress disorder in children and adolescents (Review).Evid Based Child Health. 2013 May;8(3):1004-116. doi: 10.1002/ebch.1916. Evid Based Child Health. 2013. PMID: 23877914 Review.
-
National and regional prevalence of posttraumatic stress disorder in sub-Saharan Africa: A systematic review and meta-analysis.PLoS Med. 2020 May 15;17(5):e1003090. doi: 10.1371/journal.pmed.1003090. eCollection 2020 May. PLoS Med. 2020. PMID: 32413027 Free PMC article.
Cited by
-
How COVID-19 shaped mental health: from infection to pandemic effects.Nat Med. 2022 Oct;28(10):2027-2037. doi: 10.1038/s41591-022-02028-2. Epub 2022 Oct 3. Nat Med. 2022. PMID: 36192553 Free PMC article. Review.
-
[Skills fOr Life Adjustment and Resilience Program].Psychotherapeut (Berl). 2021;66(6):533-542. doi: 10.1007/s00278-021-00535-0. Epub 2021 Sep 15. Psychotherapeut (Berl). 2021. PMID: 34539085 Free PMC article. German.
-
Strategies for Delivering Mental Health Services in Response to Global Climate Change: A Narrative Review.Int J Environ Res Public Health. 2020 Nov 18;17(22):8562. doi: 10.3390/ijerph17228562. Int J Environ Res Public Health. 2020. PMID: 33218141 Free PMC article. Review.
-
A Copernican Approach to Brain Advancement: The Paradigm of Allostatic Orchestration.Front Hum Neurosci. 2019 Apr 26;13:129. doi: 10.3389/fnhum.2019.00129. eCollection 2019. Front Hum Neurosci. 2019. PMID: 31105539 Free PMC article.
-
Coronavirus disease 2019 (COVID-19) and global mental health.Glob Health J. 2021 Mar;5(1):31-36. doi: 10.1016/j.glohj.2021.02.004. Epub 2021 Feb 13. Glob Health J. 2021. PMID: 33614179 Free PMC article. Review.
References
-
- Redlener I, Reilly MJ. Lessons from Sandy—preparing health systems for future disasters. N Engl J Med. 2012;367(24):2269-2271. - PubMed
-
- Recovery NYC. Community development block grant disaster recovery: the City of New York action plan incorporating amendments 1-11. http://www.nyc.gov/html/cdbg/downloads/pdf/cdbg-dr_action_plan_incorpora.... Published February 1, 2016. Accessed August 23, 2017.
-
- National Oceanic and Atmospheric Administration, US Dept of Commerce Service assessment: Hurricane/post-Tropical Cyclone Sandy, October 22-29, 2012. https://www.weather.gov/media/publications/assessments/Sandy13.pdf. Published May 2013. Accessed August 23, 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
