

MRI for adenomyosis: a pictorial review
- PMID: 28980163
- PMCID: PMC5707223
- DOI: 10.1007/s13244-017-0576-z
MRI for adenomyosis: a pictorial review
Abstract
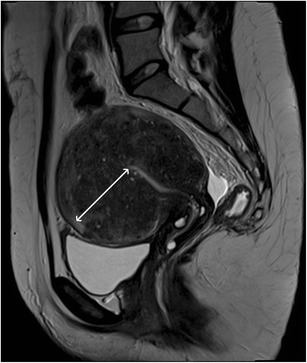
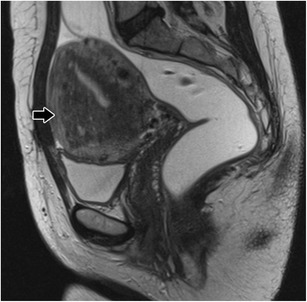
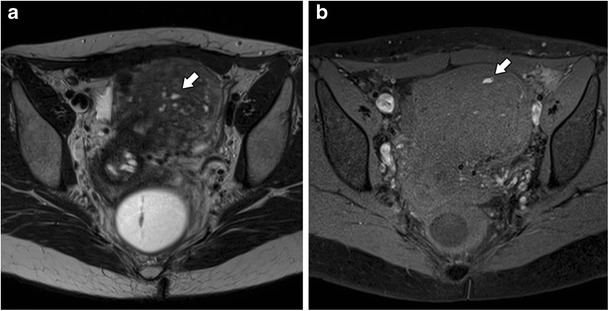
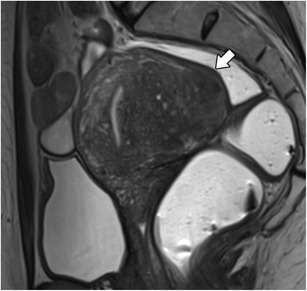
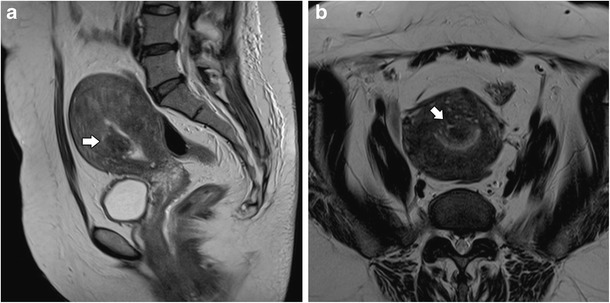
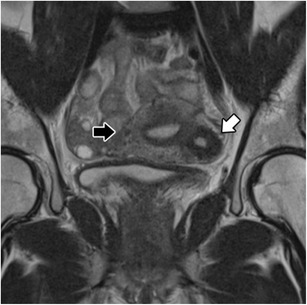
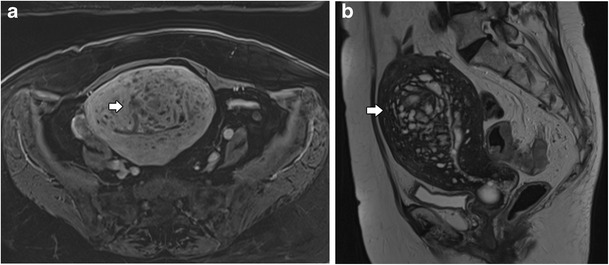
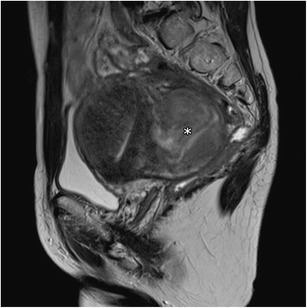
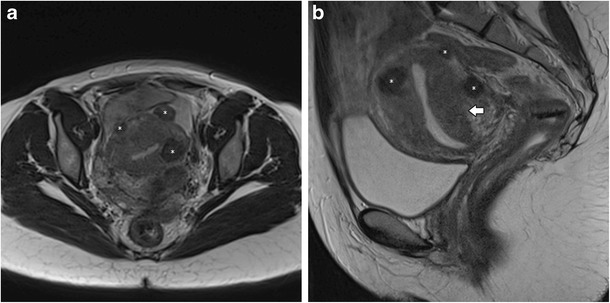
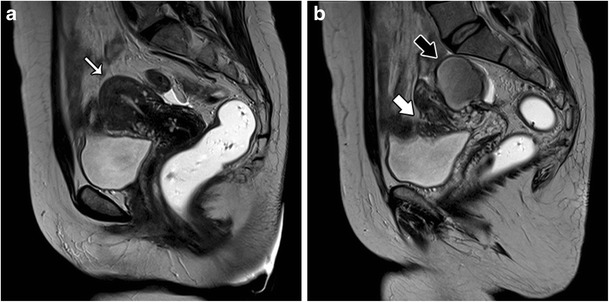
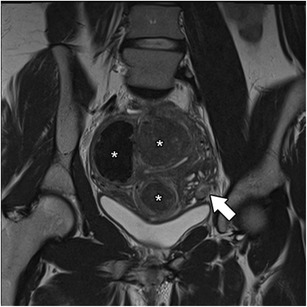
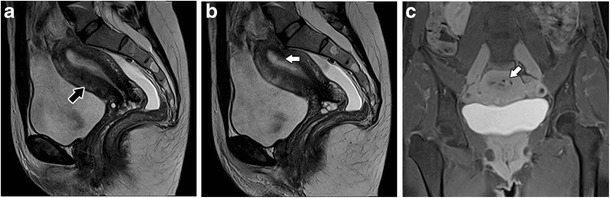
Adenomyosis is defined as the presence of ectopic endometrial glands and stroma within the myometrium. It is a disease of the inner myometrium and results from infiltration of the basal endometrium into the underlying myometrium. Transvaginal ultrasonography (TVUS) and magnetic resonance imaging (MRI) are the main radiologic tools for this condition. A thickness of the junctional zone of at least 12 mm is the most frequent MRI criterion in establishing the presence of adenomyosis. Adenomyosis can appear as a diffuse or focal form. Adenomyosis is often associated with hormone-dependent lesions such as leiomyoma, deep pelvic endometriosis and endometrial hyperplasia/polyps. Herein, we illustrate the MRI findings of adenomyosis and associated conditions, focusing on their imaging pitfalls.
Teaching points: • Adenomyosis is defined as the presence of ectopic endometrium within the myometrium. • MRI is an accurate tool for the diagnosis of adenomyosis and associated conditions. • Adenomyosis can be diffuse or focal. • The most established MRI finding is thickening of junctional zone exceeding 12 mm. • High-signal intensity myometrial foci on T2- or T1-weighted images are also characteristic.
Keywords: Adenomyosis · Uterus · Female urogenital diseases · Magnetic resonance imaging · Diagnostic imaging.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
