

Fluctuations in episodic and chronic migraine status over the course of 1 year: implications for diagnosis, treatment and clinical trial design
- PMID: 28980171
- PMCID: PMC5628086
- DOI: 10.1186/s10194-017-0787-1
Fluctuations in episodic and chronic migraine status over the course of 1 year: implications for diagnosis, treatment and clinical trial design
Abstract
Background: Relatively little is known about the stability of a diagnosis of episodic migraine (EM) or chronic migraine (CM) over time. This study examines natural fluctuations in self-reported headache frequency as well as the stability and variation in migraine type among individuals meeting criteria for EM and CM at baseline.
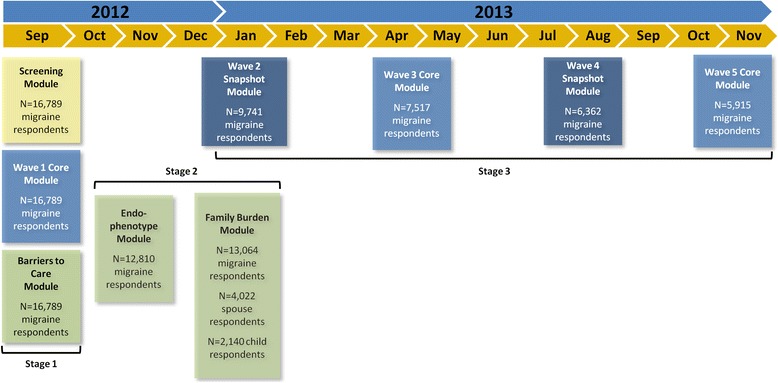
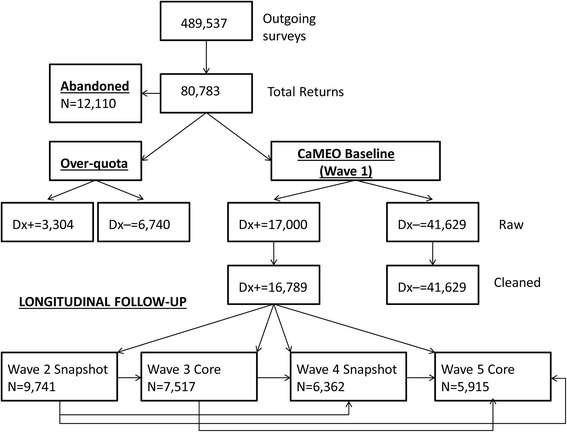
Methods: The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study was a longitudinal survey of US adults with EM and CM identified by a web-questionnaire. A validated questionnaire was used to classify respondents with EM (<15 headache days/month) or CM (≥15 headache days/month) every three months for a total of five assessments. We described longitudinal persistence of baseline EM and CM classifications. In addition, we modelled longitudinal variation in headache day frequency per month using negative binomial repeated measures regression models (NBRMR).
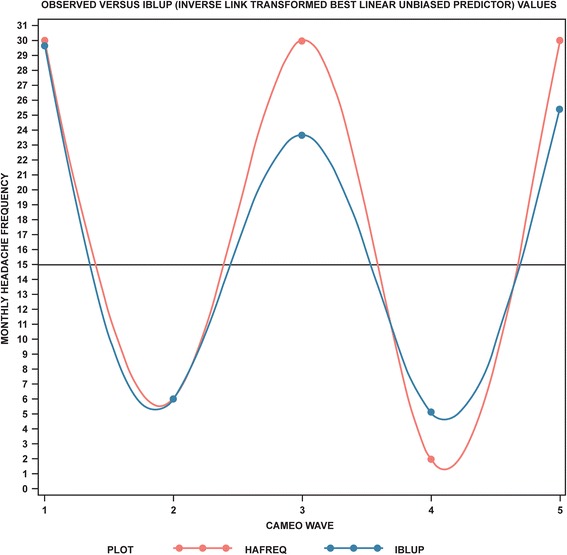
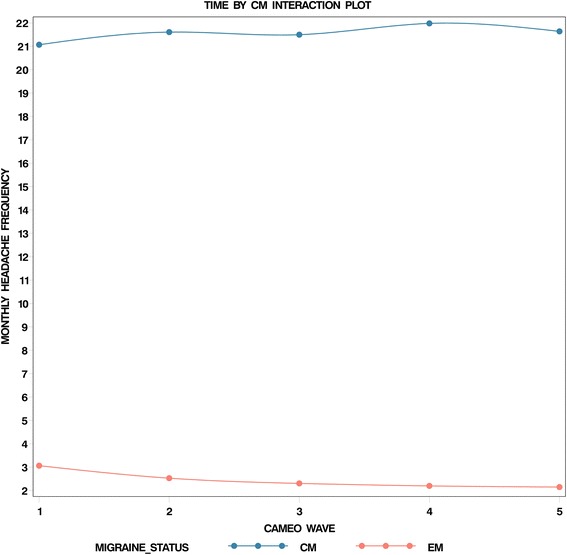
Results: Among the 5464 respondents with EM at baseline providing four or five waves of data, 5048 (92.4%) had EM in all waves and 416 (7.6%) had CM in at least one wave. Among 526 respondents with CM at baseline providing four or five waves of data, 140 (26.6%) had CM in every wave and 386 (73.4%) had EM for at least one wave. Individual plots revealed striking within-person variations in headache days per month. The NBRMR model revealed that the rate of headache days increased across waves of observation 19% more per wave for CM compared to EM (rate ratio [RR], 1.19; 95% CI, 1.13-1.26). After adjustment for covariates, the relative difference changed to a 26% increase per wave (RR, 1.26; 95% CI, 1.2-1.33).
Conclusions: Follow-up at three-month intervals reveals a high level of short-term variability in headache days per month. As a consequence, many individuals cross the CM diagnostic boundary of ≥15 headache days per month.Nearly three quarters of persons with CM at baseline drop below this diagnostic boundary at least once over the course of a year. These findings are of interest in the consideration of headache classification and diagnosis, the design and interpretation of epidemiologic and clinical studies, and clinical management.
Keywords: Chronic migraine; Episodic migraine; Longitudinal; Migraine; Remission.
Conflict of interest statement
Competing interests
Daniel Serrano is an employee of Endpoint Outcomes. This work was initiated while he was serving as a consultant for Vedanta Research and completed while Associate Director of Psychometrics at Endpoint Outcomes. He has received support funded by Allergan plc, CoLucid, Endo Pharmaceuticals, GlaxoSmithKline, MAP Pharmaceuticals, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation. In addition, he has received funding from Allergan plc, Astellas, Genenteck, Lumena, Neurocrine, Shire and Supernus. Richard B. Lipton serves on the editorial board of
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Headache Classification Committee of the International Headache Society (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33:629–808. doi:10.1177/0333102413485658 - PubMed
-
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M (2001) Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 41:646–657 - PubMed
-
- Buse DC, Manack AN, Fanning KM, Serrano D, Reed ML, Turkel CC, Lipton RB (2012) Chronic migraine prevalence, disability, and sociodemographic factors: results from the American Migraine Prevalence and Prevention Study. Headache 52:1456–1470. doi:10.1111/j.1526-4610.2012.02223.x - PubMed
-
- Blumenfeld AM, Varon SF, Wilcox TK, Buse DC, Kawata AK, Manack A, Goadsby PJ, Lipton RB (2011) Disability, HRQoL and resource use among chronic and episodic migraineurs: results from the International Burden of Migraine Study (IBMS). Cephalalgia 31:301–315. doi:10.1177/0333102410381145 - PubMed
-
- Payne KA, Varon SF, Kawata AK, Yeomans K, Wilcox TK, Manack A, Buse DC, Lipton RB, Goadsby PJ, Blumenfeld AM (2011) The International Burden of Migraine Study (IBMS): study design, methodology, and baseline cohort characteristics. Cephalalgia 31:1116–1130. doi:10.1177/0333102411410610 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
