

Blood pressure and in-hospital outcomes in patients presenting with ischaemic stroke
- PMID: 28982227
- PMCID: PMC5837595
- DOI: 10.1093/eurheartj/ehx330
Blood pressure and in-hospital outcomes in patients presenting with ischaemic stroke
Abstract
Aims: Post-stroke hypertension is associated with poor short-term outcome, although the results have been conflicting. Our objective was to evaluate the association of blood pressure (BP) and in-hospital outcomes in patients with acute ischaemic stroke.
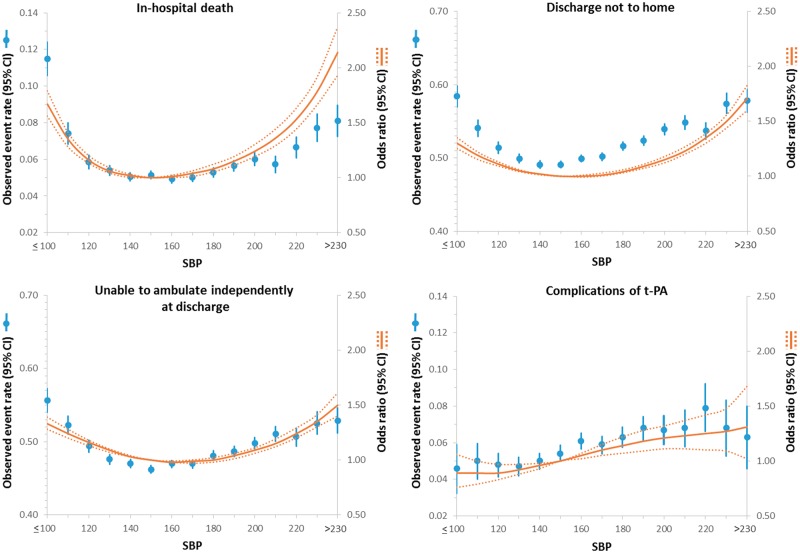
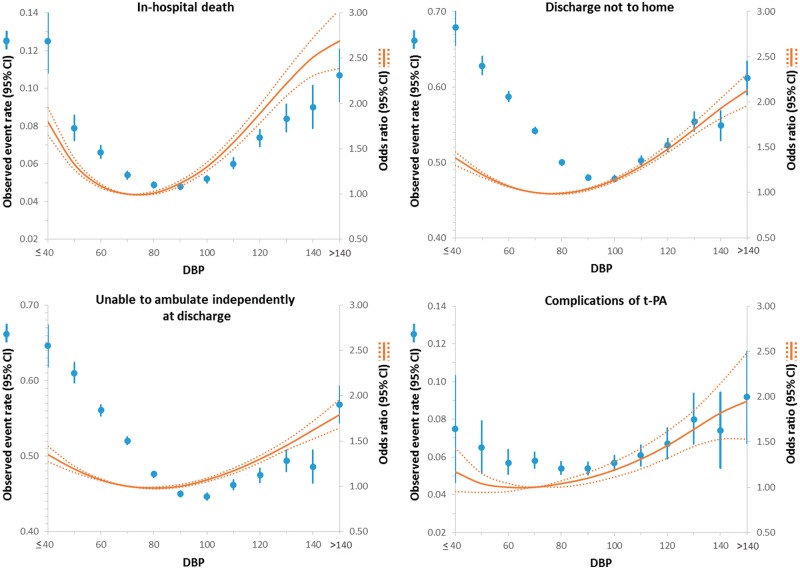
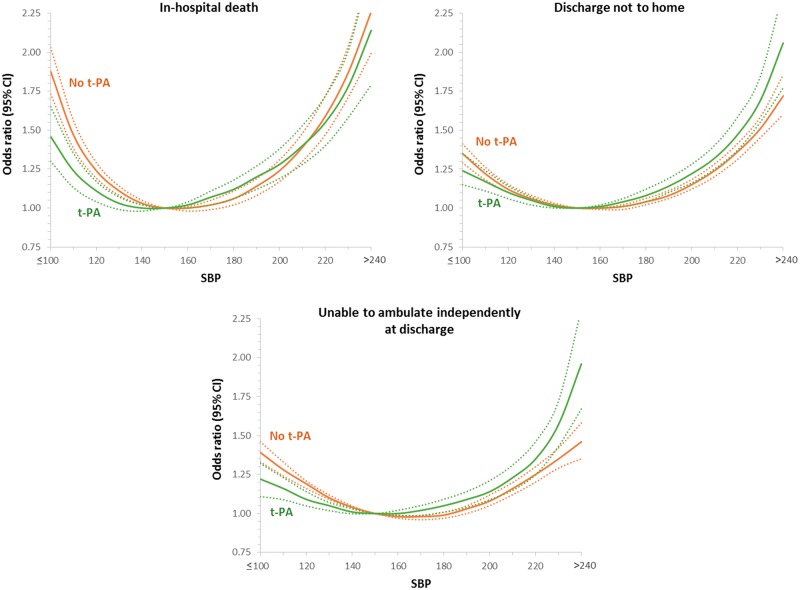
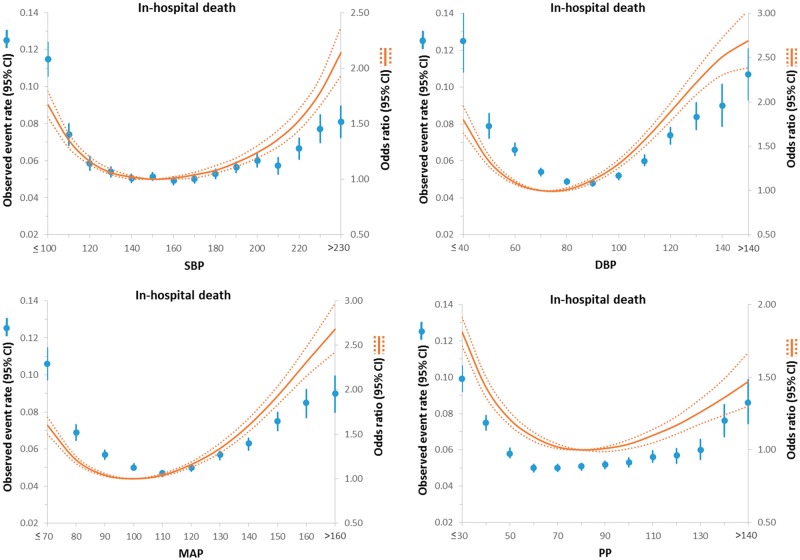
Methods and results: Patients in the Get With The Guidelines-Stroke registry with acute ischaemic stroke were included. Admission systolic and diastolic BP was used to compute mean arterial pressure (MAP) and pulse pressure (PP). The outcomes of interest were: in-hospital mortality, not discharged home, inability to ambulate independently at discharge and haemorrhagic complications due to thrombolytic therapy. A total of 309 611 patients with an ischaemic stroke were included. There was a J-shaped/U-shaped relationship between systolic BP and outcomes. Both lower and higher systolic BP values, compared with a central reference value, had higher risk of in-hospital death [e.g. adjusted odds ratio (95% confidence interval) (OR[CI]) = 1.16[1.13-1.20] for 120 vs. 150 mmHg and 1.24[1.19-1.30] for 200 vs. 150 mmHg], not discharged home (OR[CI] = 1.11[1.09-1.13] for 120 vs. 150 mmHg and 1.15[1.12-1.18] for 200 vs. 150 mmHg), inability to ambulate independently at discharge (OR[CI] = 1.16[1.13-1.18] for 120 vs. 150 mmHg and 1.09[1.06-1.11] for 200 vs. 150 mmHg). However, risk of haemorrhagic complications of thrombolytic therapy was lower with lower systolic BP (OR[CI] = 0.89[0.83-0.97] for 120 vs. 150 mmHg), while higher with higher systolic BP (OR[CI] = 1.21[1.11-1.32] for 200 vs. 150 mmHg). The results were largely similar for admission diastolic BP, MAP, and PP.
Conclusion: In patients hospitalized with ischaemic stroke, J-shaped, or U-shaped relationships were observed between BP variables and short-term outcomes. However, haemorrhagic complications with thrombolytic therapy were lower with lower BP.
Keywords: Blood pressure; Diastolic; Ischaemic stroke; Mean arterial pressure; Pulse pressure; Stroke; Systolic; Transient ischaemic attack.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2017. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Finding ideal blood pressure targets in ischaemic stroke: prospective insight or retrospective guesswork?Eur Heart J. 2017 Oct 1;38(37):2836-2837. doi: 10.1093/eurheartj/ehx415. Eur Heart J. 2017. PMID: 28982229 No abstract available.
References
-
- Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F, Redon J, Dominiczak A, Narkiewicz K, Nilsson PM, Burnier M, Viigimaa M, Ambrosioni E, Caufield M, Coca A, Olsen MH, Schmieder RE, Tsioufis C, van de Borne P, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Clement DL, Coca A, Gillebert TC, Tendera M, Rosei EA, Ambrosioni E, Anker SD, Bauersachs J, Hitij JB, Caulfield M, De Buyzere M, De Geest S, Derumeaux GA, Erdine S, Farsang C, Funck-Brentano C, Gerc V, Germano G, Gielen S, Haller H, Hoes AW, Jordan J, Kahan T, Komajda M, Lovic D, Mahrholdt H, Olsen MH, Ostergren J, Parati G, Perk J, Polonia J, Popescu BA, Reiner Z, Ryden L, Sirenko Y, Stanton A, Struijker-Boudier H, Tsioufis C, van de Borne P, Vlachopoulos C, Volpe M, Wood DA.. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013;34:2159–2219. - PubMed
-
- Yatsu FM, Zivin J.. Hypertension in acute ischemic strokes. Not to treat. Arch Neurol 1985;42:999–1000. - PubMed
-
- Leonardi-Bee J, Bath PM, Phillips SJ, Sandercock PA.. Group ISTC. Blood pressure and clinical outcomes in the International Stroke Trial. Stroke 2002;33:1315–1320. - PubMed
-
- Bowes MP, Zivin JA, Thomas GR, Thibodeaux H, Fagan SC.. Acute hypertension, but not thrombolysis, increases the incidence and severity of hemorrhagic transformation following experimental stroke in rabbits. Exp Neurol 1996;141:40–46. - PubMed
-
- O'Brien MD, Jordan MM, Waltz AG.. Ischemic cerebral edema and the blood-brain barrier. Distributions of pertechnetate, albumin, sodium, and antipyrine in brains of cats after occlusion of the middle cerebral artery. Arch Neurol 1974;30:461–465. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
