

Role of Cardiac Magnetic Resonance in the Diagnosis and Prognosis of Nonischemic Cardiomyopathy
- PMID: 28982571
- PMCID: PMC5708889
- DOI: 10.1016/j.jcmg.2017.08.005
Role of Cardiac Magnetic Resonance in the Diagnosis and Prognosis of Nonischemic Cardiomyopathy
Abstract
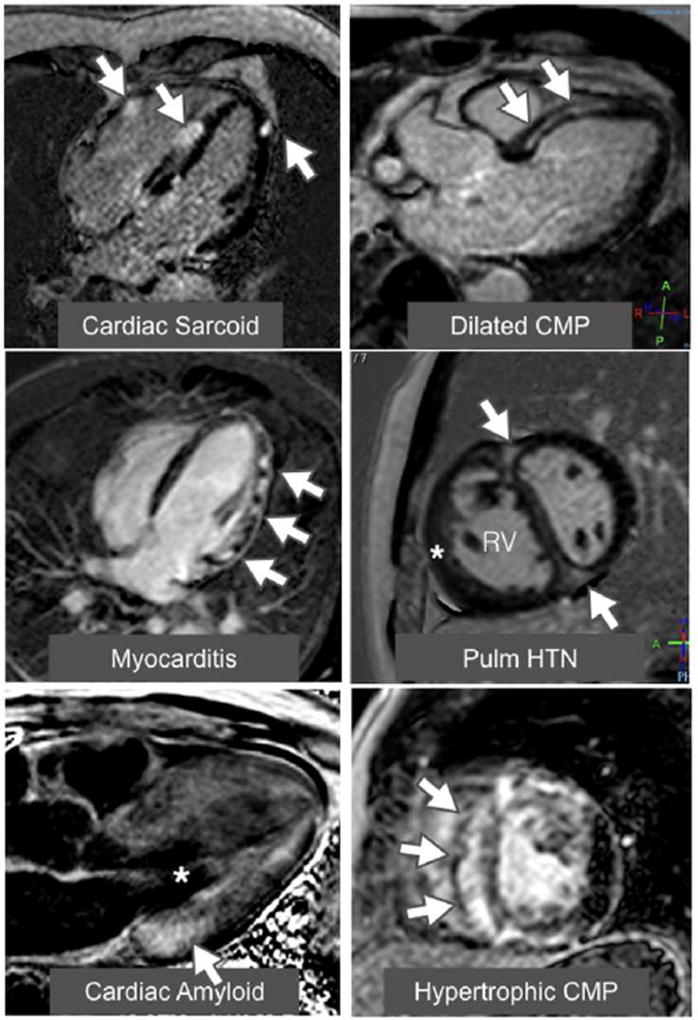
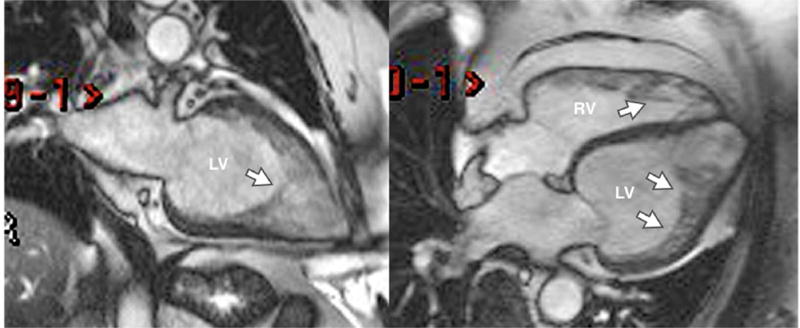
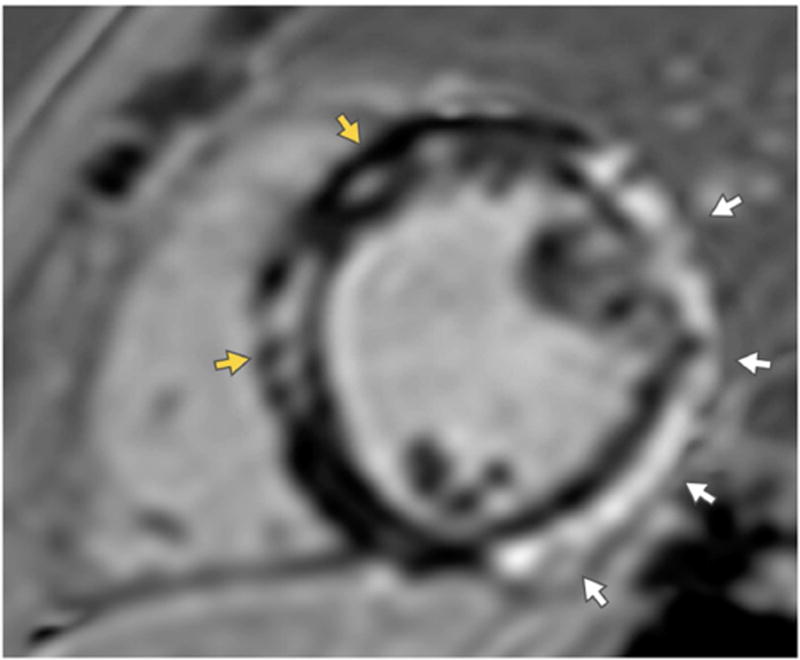
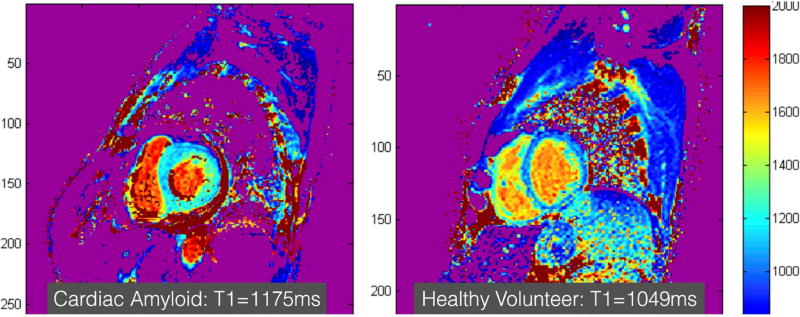
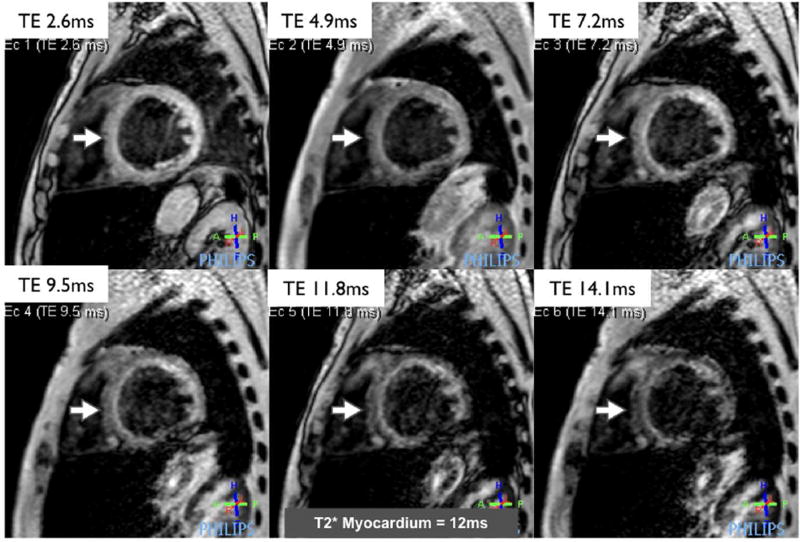
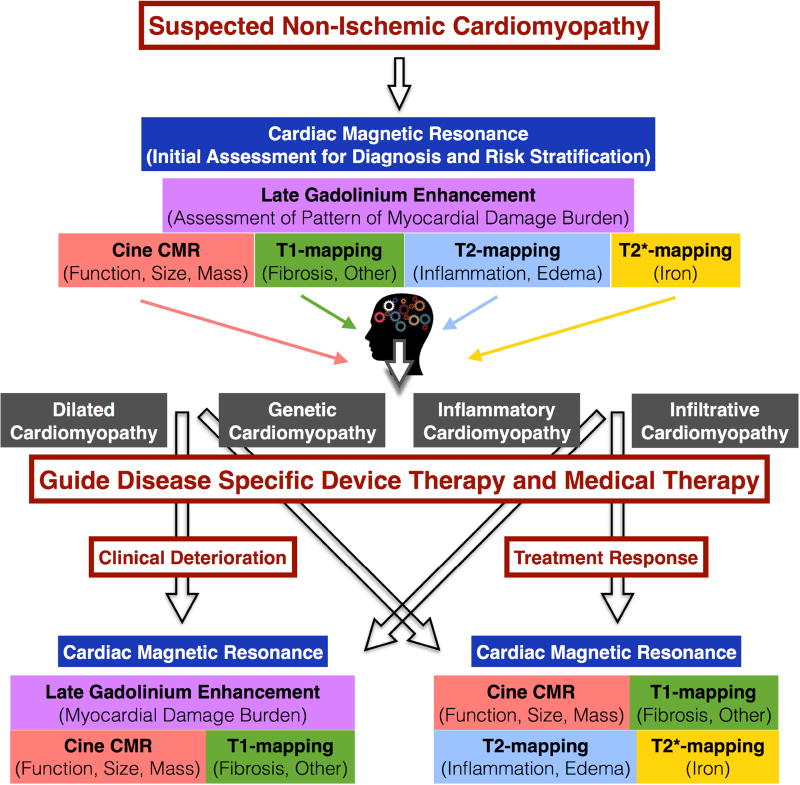
Cardiac magnetic resonance (CMR) is a valuable tool for the evaluation of patients with, or at risk for, heart failure and has a growing impact on diagnosis, clinical management, and decision making. Through its ability to characterize the myocardium by using multiple different imaging parameters, it provides insight into the etiology of the underlying heart failure and its prognosis. CMR is widely accepted as the reference standard for quantifying chamber size and ejection fraction. Additionally, tissue characterization techniques such as late gadolinium enhancement (LGE) and other quantitative parameters such as T1 mapping, both native and with measurement of extracellular volume fraction; T2 mapping; and T2* mapping have been validated against histological findings in a wide range of clinical scenarios. In particular, the pattern of LGE in the myocardium can help determine the underlying etiology of the heart failure. The presence and extent of LGE determine prognosis in many of the nonischemic cardiomyopathies. The use of CMR should increase as its utility in characterization and assessment of prognosis in cardiomyopathies is increasingly recognized.
Keywords: amyloidosis; cardiomyopathy; cardiovascular magnetic resonance; heart failure; hypertrophic cardiomyopathy; sarcoidosis.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Arbustini E, Narula N, Tavazzi L, et al. The MOGE(S) classification of cardiomyopathy for clinicians. Journal of the American College of Cardiology. 2014;64:304–18. - PubMed
-
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. The New England journal of medicine. 2014;371:993–1004. - PubMed
-
- Iles LM, Ellims AH, Llewellyn H, et al. Histological validation of cardiac magnetic resonance analysis of regional and diffuse interstitial myocardial fibrosis. European heart journal cardiovascular Imaging. 2015;16:14–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
