

Association between in-hospital guideline adherence and postdischarge major adverse outcomes of patients with acute coronary syndrome in Vietnam: a prospective cohort study
- PMID: 28982823
- PMCID: PMC5640016
- DOI: 10.1136/bmjopen-2017-017008
Association between in-hospital guideline adherence and postdischarge major adverse outcomes of patients with acute coronary syndrome in Vietnam: a prospective cohort study
Abstract
Objective: We aimed to determine the association between physician adherence to prescribing guideline-recommended medications during hospitalisation and 6-month major adverse outcomes of patients with acute coronary syndrome in Vietnam.
Design: Prospective cohort study.
Setting: The study was carried out in two public hospitals in Vietnam between January and October 2015. Patients were followed for 6 months after discharge.
Participants: Patients who survived during hospitalisation with a discharge diagnosis of acute coronary syndrome and who were eligible for receiving at least one of the four guideline-recommended medications.
Exposures: Guideline adherence was defined as prescribing all guideline-recommended medications at both hospital admission and discharge for eligible patients. Medications were antiplatelet agents, beta-blockers, ACE inhibitors or angiotensin II receptor blockers and statins.
Main outcome measure: Six-month major adverse outcomes were defined as all-cause mortality or hospital readmission due to cardiovascular causes occurring during 6 months after discharge. Cox regression models were used to estimate the association between guideline adherence and 6-month major adverse outcomes.
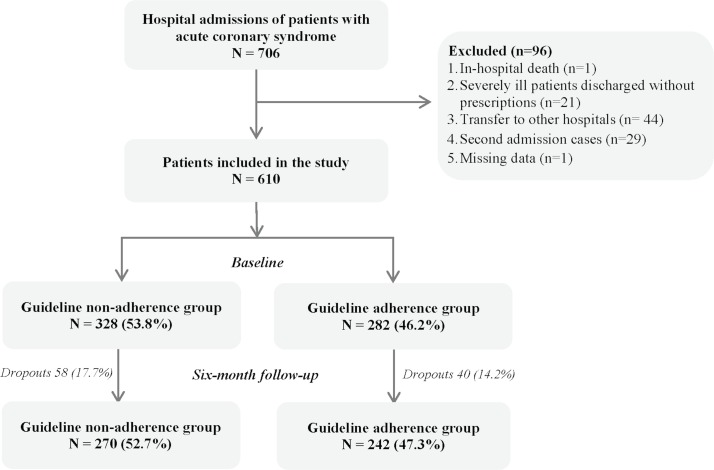
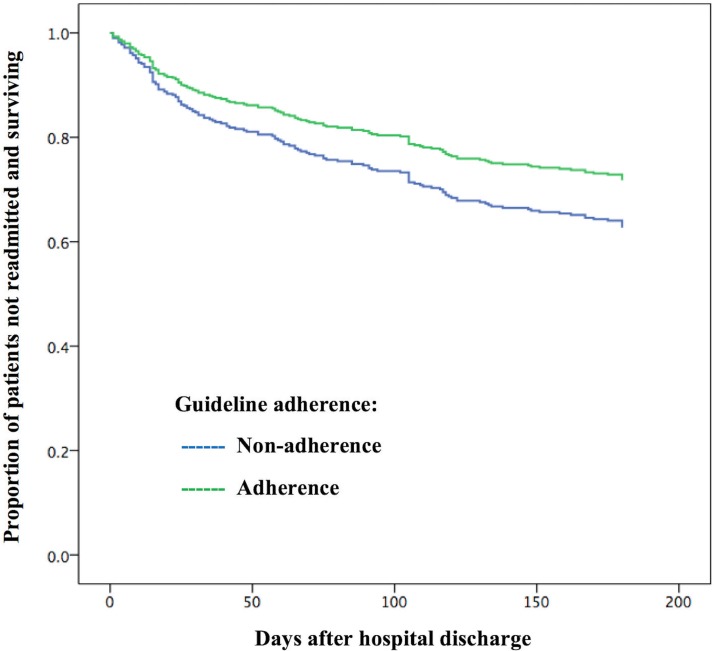
Results: Overall, 512 patients were included. Of those, there were 242 patients (47.3%) in the guideline adherence group and 270 patients (52.3%) in the non-adherence group. The rate of 6-month major adverse outcomes was 30.5%. A 29% reduction in major adverse outcomes at 6 months after discharge was found for patients of the guideline adherence group compared with the non-adherence group (adjusted HR, 0.71; 95% CI, 0.51 to 0.98; p=0.039). Covariates significantly associated with the major adverse outcomes were percutaneous coronary intervention, prior heart failure and renal insufficiency.
Conclusions: In-hospital guideline adherence was associated with a significant decrease in major adverse outcomes up to 6 months after discharge. It supports the need for improving adherence to guidelines in hospital practice in low-income and middle-income countries like Vietnam.
Keywords: Guideline Adherence; Ischaemic Heart Disease; Major Adverse Outcomes; Prescribing.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Utilization of Evidence-Based Secondary Prevention Medications at the Time of Discharge in Patients with Acute Coronary Syndrome (ACS) in Qatar.Curr Vasc Pharmacol. 2016;14(4):394-403. doi: 10.2174/1570161114666160226150336. Curr Vasc Pharmacol. 2016. PMID: 26916397
-
Optimizing prevention and guideline-concordant care in Montenegro.Int J Cardiol. 2016 Aug;217 Suppl:S32-6. doi: 10.1016/j.ijcard.2016.06.218. Epub 2016 Jun 28. Int J Cardiol. 2016. PMID: 27381861
-
Prescribing patterns of evidence-based heart failure pharmacotherapy and outcomes in the ASIAN-HF registry: a cohort study.Lancet Glob Health. 2018 Sep;6(9):e1008-e1018. doi: 10.1016/S2214-109X(18)30306-1. Lancet Glob Health. 2018. PMID: 30103979
-
Effect of evidence-based cardiac drug therapy on mortality in patients with acute coronary syndrome: Findings from the Gulf COAST registry.Cardiovasc Ther. 2018 Dec;36(6):e12463. doi: 10.1111/1755-5922.12463. Epub 2018 Aug 28. Cardiovasc Ther. 2018. PMID: 30079461
-
Patient Adherence to Secondary Prevention Therapies After an Acute Coronary Syndrome: A Scoping Review.Clin Ther. 2023 Nov;45(11):1119-1126. doi: 10.1016/j.clinthera.2023.08.011. Epub 2023 Sep 9. Clin Ther. 2023. PMID: 37690915
Cited by
-
Addressing adherence challenges in long-term statin treatment among Asian populations: Current gaps and proposed solutions.Am J Prev Cardiol. 2025 Jun 2;23:101019. doi: 10.1016/j.ajpc.2025.101019. eCollection 2025 Sep. Am J Prev Cardiol. 2025. PMID: 40606516 Free PMC article. Review.
-
Association between Adherence to Guideline-Recommended Preventive Medications and In-Hospital Mortality among Non-Reperfused ST-Elevation Myocardial Infarction Patients Admitted to a Tertiary Care Academic Center in a Developing Country.Glob Heart. 2020 Feb 6;15(1):8. doi: 10.5334/gh.394. Glob Heart. 2020. PMID: 32489781 Free PMC article.
-
Adherence of cardiologist physicians to the American Heart Association guideline in approach to risk factors of cardiovascular diseases: An experience from a teaching hospital.ARYA Atheroscler. 2019 Jan;15(1):38-43. doi: 10.22122/arya.v15i1.1774. ARYA Atheroscler. 2019. PMID: 31440284 Free PMC article.
-
Adherence to Prescribing Guideline-Directed Medical Therapy at Hospital Discharge in Subjects With Acute Coronary Syndrome, and the Relationship With Mortality.Cureus. 2022 Apr 10;14(4):e24000. doi: 10.7759/cureus.24000. eCollection 2022 Apr. Cureus. 2022. PMID: 35547465 Free PMC article.
-
Adherence to Cardiovascular Prevention Guidelines in an Academic Centre.CJC Open. 2023 Mar 23;5(7):530-536. doi: 10.1016/j.cjco.2023.03.010. eCollection 2023 Jul. CJC Open. 2023. PMID: 37496787 Free PMC article.
References
-
- World Health Organization. The top 10 causes of death. 2017, 2017.
-
- Vietnam Ministry of Health. Vietnam health statistical profile 2009-2013. Vietnam Ministry of Health 2013.
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. . AHA/ACC Guideline for the management of patients with non-ST-elevation acute coronary syndromes. Circulation 2014;426:130:e344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous