

Measles outbreak investigation in Guji zone of Oromia Region, Ethiopia
- PMID: 28983397
- PMCID: PMC5619924
- DOI: 10.11604/pamj.supp.2017.27.2.10705
Measles outbreak investigation in Guji zone of Oromia Region, Ethiopia
Abstract
Introduction: Despite the increase of immunization coverage (administrative) of measles in the country, there are widespread outbreaks of measles. In this respect, we investigated one of the outbreaks that occurred in hard to reach kebeles of Guji Zone, Oromia region, to identify the contributing factors that lead to the protracted outbreak of measles.
Methods: We used a cross-sectional study design to investigate a measles outbreak in Guji zone, Oromia region. Data entry and analysis was performed using EPI-Info version 7.1.0.6 and MS-Microsoft Excel.
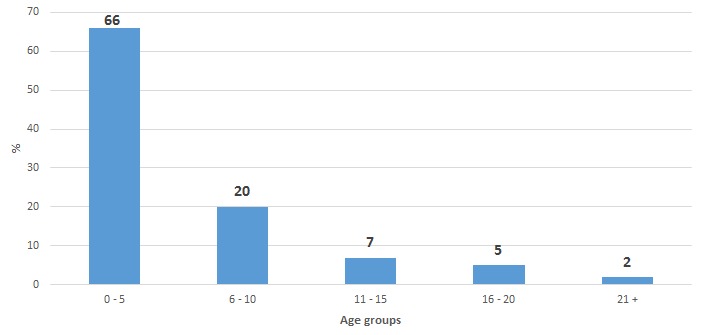
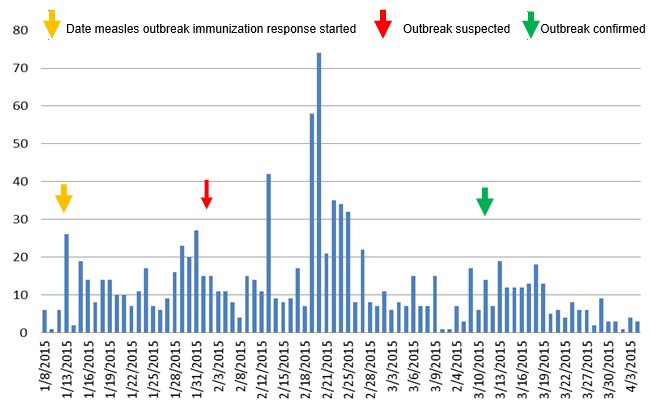
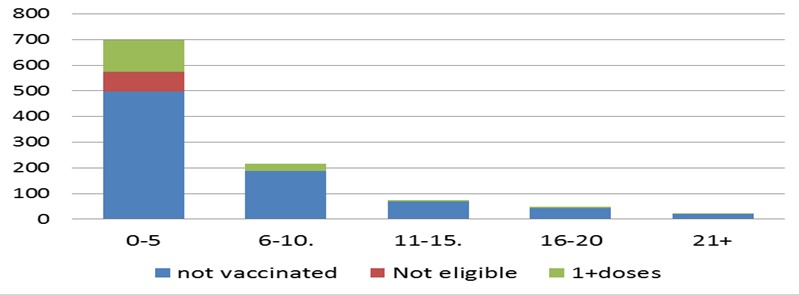
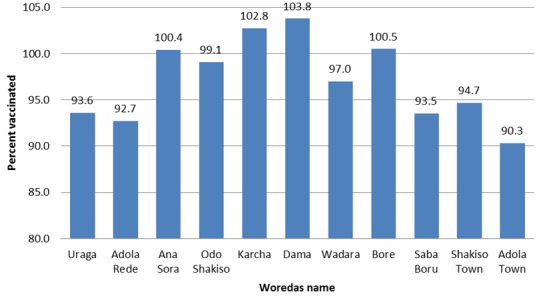
Results: In three months' time a total of 1059 suspected cases and two deaths were reported from 9 woredas affected by a measles outbreak in Guji zone. The cumulative attack rate of 81/100,000 population and case fatality ratio of 0.2% was recorded. Of these, 821 (77.5%) cases were < 15 years of age, and 742 (70%) were zero doses of measles vaccine. Although, all age groups were affected under five years old were more affected 495 (48%) than any other age groups. In response to the outbreak, an outbreak response immunization was organized at the 11th week of the epidemic, when the epidemic curve started to decline. 6 months to14 years old were targeted for outbreak response immunization and the overall coverage was 97 % (range: 90-103%). Case management with vitamin A supplementation, active case search, and health education was some of the activities carried out to curb the outbreak.
Conclusion: We conclude that low routine immunization coverage in conjunction with low access to routine immunization in hard to reach areas, low community awareness in utilization of immunization service, inadequate cold chain management and delivery of a potent vaccine in hard to reach woredas/kebeles were likely contributed to the outbreak that's triggered a broad spread epidemic affecting mostly children without any vaccination. We also figured that the case-based surveillance lacks sensitivity and timely confirmation of the outbreak, which as a result outbreak response immunization were delayed. We recommend establishing reaching every child (REC) strategy in Guji zone with particular emphasis too hard reach areas to enhance the current immunization service, and furthermore to conduct data quality self-assessment or cluster coverage survey to verify the reported high vaccination coverage in some kebeles. We also recommend conducting the second opportunity as a form of supplemental immunization activities in 2-3 year interval or consider the national second dose introduction in the routine immunization system to improve population immunity. We further recommend that there is a need to boost the sensitivity of case-based surveillance system to be able to early detect, confirm and react to future epidemics.
Keywords: Ethiopia; Measles; outbreak investigation; outbreak management; outbreak response.
Figures
References
-
- Masresha BG, Fall A, Eshetu M, Sosler S, Alleman M, Goodson JL, et al. Measles mortality reduction and pre-elimination in the African Region, 2001-2009. J Infect Dis. 2011 Jul 1;204(suppl 1):S198–204. - PubMed
-
- Simons E, Ferrari M, Fricks J, Wannemuehler K, Anand A, Burton A, et al. Assessment of the 2010 global measles mortality reduction goal: results from a model of surveillance data. The Lancet. 2012;379(9832):2173–8. - PubMed
-
- Mitiku K, Bedada T, Masresha BG, Kegne W, Nafo-Traoré F, Tesfaye N, et al. Progress in measles mortality reduction in Ethiopia, 2002-2009. J Infect Dis. 2011 Jul 1;204(suppl 1):S232–8. - PubMed
-
- CDC . Measles - Horn of Africa, 2010-2011. Accessed on September 24, 2016.
-
- Yaméogo KR, Perry RT, Yaméogo A, Kambiré C, Kondé MK, Nshimirimana D, et al. Migration as a risk factor for measles after a mass vaccination campaign, Burkina Faso, 2002. Int J Epidemiol. 2005;34(3):556–64. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
