

Contrast-enhanced ultrasound (CEUS) of the abdominal vasculature
- PMID: 28983674
- PMCID: PMC5884912
- DOI: 10.1007/s00261-017-1329-7
Contrast-enhanced ultrasound (CEUS) of the abdominal vasculature
Abstract
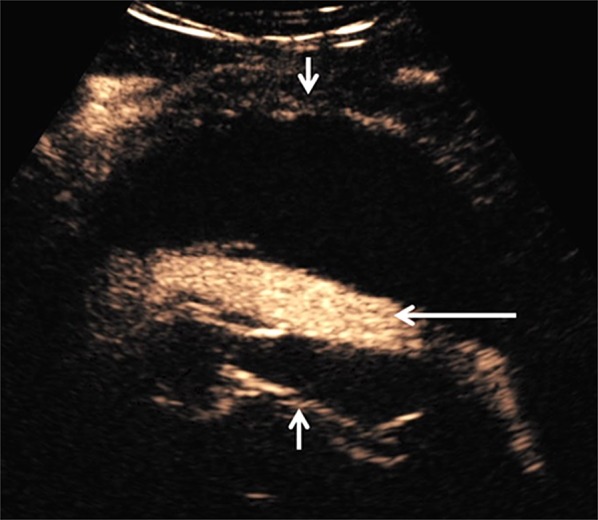
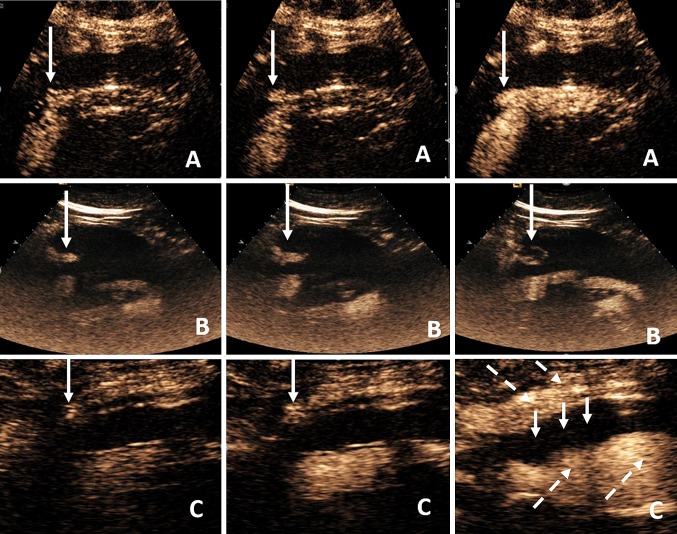
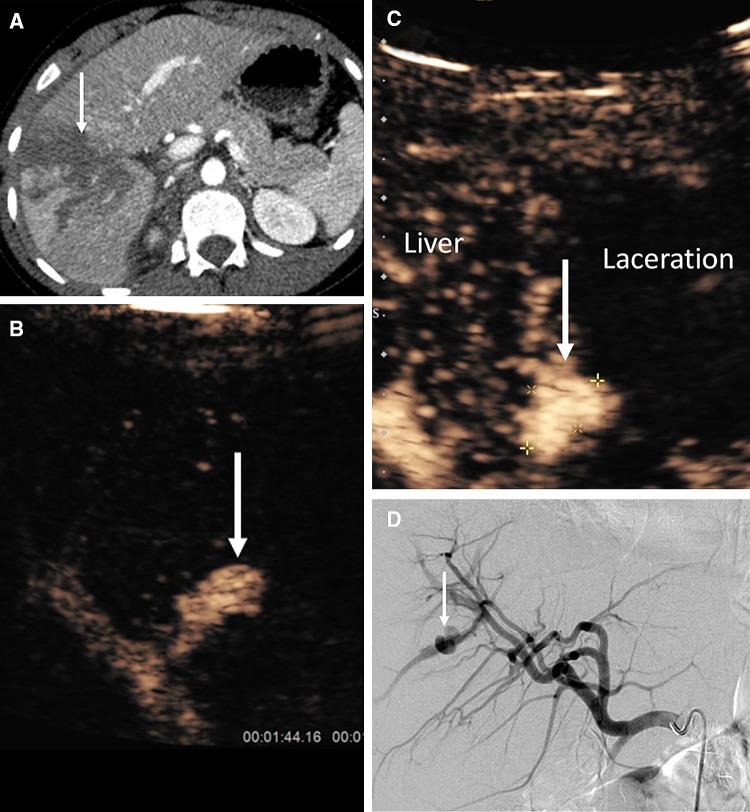
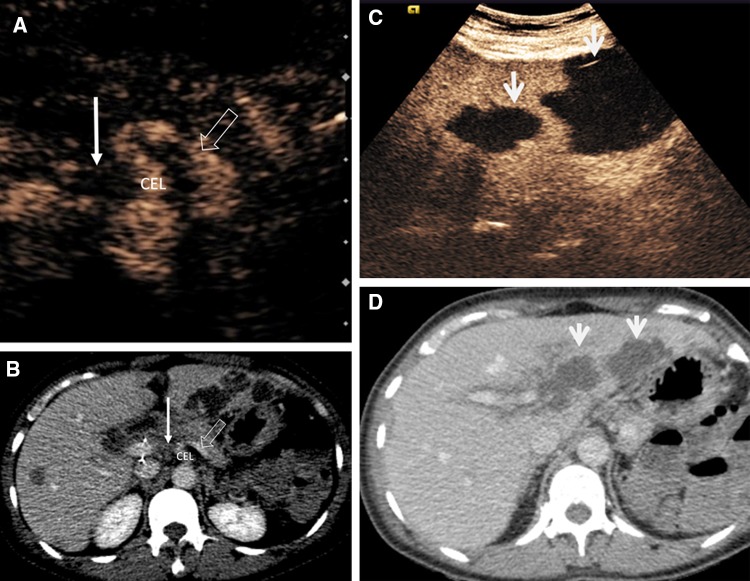
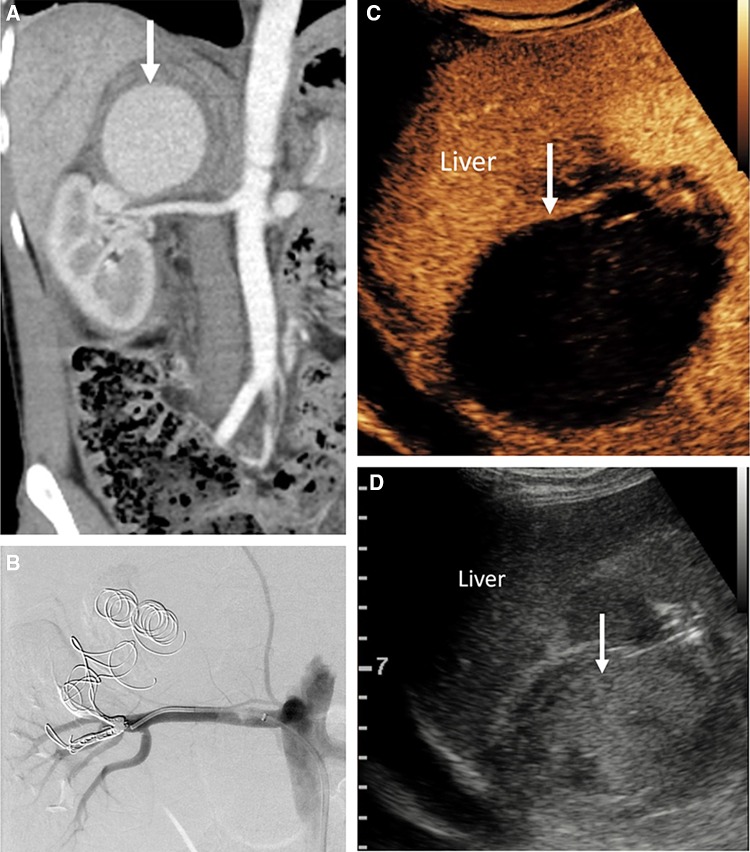
Vascular diseases account for a significant proportion of abdominal pathology and represent a common referral source for abdominal ultrasonographic examinations. B-mode, color Doppler, and spectral Doppler analyses are well-established in the evaluation of abdominal blood vessels although they may occasionally be limited by lower sensitivity for slow flow visualization or the deeper location of abdominal vascular structures. The introduction of microbubbles as ultrasonographic contrast agents has rendered contrast-enhanced ultrasound (CEUS), a valuable complementary ultrasonographic technique, which is capable of addressing clinically significant problems and guiding patient management. The purpose of this pictorial review is to analyze the use of CEUS in the evaluation of abdominal vascular pathology and illustrate such applications by presenting representative images. Pathology discussed includes abdominal aortic aneurysm, post-endovascular treatment aorta, portal vein thrombosis, abdominal vascular trauma, and organ transplantation along with its complications.
Keywords: Aneurysm; Aorta; Contrast-enhanced ultrasound; Endoleak; Portal vein; Trauma.
Conflict of interest statement
Funding
Not applicable.
Conflict of interest
Authors VR and CF declare that they have no potential conflict of interest. Author GY has received lecture fees from Bracco. Author DH has received fees from Bracco for providing a training workshop on CEUS. Author PS has received lecture fees from Bracco, Siemens, Samsung, Philips, and Hitachi.
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
